Welcome to our Breast & Gynecologic Cancer Program. Whether you’ve just received a new diagnosis of breast cancer, are navigating a course of therapy, living with advanced disease, have completed treatment and are participating in our survivorship program, we appreciate the opportunity to provide you with personalized, multidisciplinary and state-of-the-art care. Access to our team of experts, breakthrough treatments, the most advanced clinical trials available, and a number of support services are here to care for you and your family throughout this challenging time.
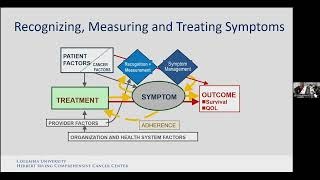
Managing the Side-Effects of Cancer Therapy
The Johns Hopkins Medicine Breast & Gynecologic Cancer Program presents a mini-symposium on managing the effects of cancer treatment. Dr Dawn Hershman from the Herbert Irving Comprehensive Columbia Cancer Center at Columbia University, Dr Kimberley Lee from the H Lee Moffitt Cancer Center at the University of South Florida, and breast cancer survivor Melissa Preston-Wesby address the aspects of managing what comes with a cancer diagnosis.
-
Advanced, Personalized Treatment
Our main goal is to decipher the mechanisms of cancer and find better ways to treat it. Conducting basic laboratory science and clinical trials puts us closer to this goal, which will allow us to provide a more individualized road map for managing each patient’s breast cancer.
-
Expert, Collaborative Care
Choose Johns Hopkins to gain access to the expertise of multiple medical professionals working together to create the best treatment plan for you—one based on evidence-based treatment standards, many of which have been pioneered by clinician-scientists here at Johns Hopkins.
-
Coordinated Support Services
Becoming a patient in our program means more than expert medical treatment. From cosmetic procedures that help you feel whole again to support groups whose members relate to your circumstances, the breadth and significance of our support services cannot be underestimated.
Integrative Medicine

The Breast Cancer Multidisciplinary Clinic
Jean Wright, M.D., Director of the Breast Cancer Multidisciplinary Clinic at the Johns Hopkins Kimmel Cancer Center and Associate Professor of Radiation Oncology and Molecular Radiation Sciences in the Johns Hopkins University School of Medicine, explains the benefits of multidisciplinary care in treating breast cancer.

Living with Metastatic Breast Cancer during COVID-19
Breast Cancer Treatment Implications for Patients Undergoing Care during COVID-19
Breast Cancer Follow-up and Survivorship Care in the Era of COVID-19