Strategies for Venous Thromboembolism Prevention
 View the full size version of the chart..
View the full size version of the chart..A Systemic Approach to Preventing Harmful Blood Clots
Delivering risk-appropriate prophylaxis to hospitalized patients can prevent up to 70 percent of venous thromboembolism (VTE) cases, according to published studies. Yet a large body of research indicates that patients do not reliably receive these treatments, in the form of anti-clotting medications, such as heparin, and mechanical devices that reduce blood clot formation. One multinational study, for example, found that 58.5 percent of surgical patients and 39.5 percent of medical patients received appropriate VTE prophylaxis.
Nearly a decade ago, The Johns Hopkins Hospital’s performance on VTE prevention measures mirrored that of other hospitals. In 2005, a chart audit of several high risk patient populations found that just 32 percent received risk-appropriate VTE prophylaxis. However, over time the hospital has gradually increased that performance to greater than 90 percent, and it continues striving for 100 percent. Below are several of the key strategies that have helped us achieve this improvement.
Service-specific VTE Order Sets
For every patient, providers must balance the risks of bleeding and clotting. They must consider risk factors, such as bone fractures and major surgery, and contraindications, such as gastrointestinal bleeding, and their treatment recommendations should be informed by the medical evidence. Giving the same VTE prophylaxis to all patients without regard for their individual factors may actually cause more harm than benefit.
As an initial intervention, the hospital’s VTE Collaborative developed order sets that were tailored to 16 different patient types, such as trauma, surgery and medicine. For each order set, algorithms help physicians to assign patients to different risk categories. Based on each patient’s risk level, providers receive guidance on which prophylaxis orders are most appropriate.
Initially, these order sets were available only in paper form. After they were introduced, performance on risk-appropriate VTE prophylaxis reached 65 percent—roughly doubling the previous rate. However, performance still fell short of the hospital’s goal. There were no “hard stops” to ensure that patients’ risk of blood clots was considered by physicians, who often felt that completing the forms was burdensome.
Mandatory VTE Risk Assessment and Computerized Clinical Decision Support
To ingrain VTE prophylaxis assessments into clinicians’ workflow, the hospital built service-specific order sets into the computerized provider order-entry system. A mandatory screen guides clinicians to select risk factors and contraindications, while the system also pulls in data from the electronic record to make the risk assessment and issue recommended orders. This risk assessment is required, but physicians can still choose to deviate from the recommendation based on other clinical considerations. With the addition of computerized clinical decision support, the hospital’s performance on ordering appropriate prophylaxis increased substantially, with rates generally between 80 percent and 90 percent.
These improvement efforts were detailed in a June 2012 BMJ article, and recently an update in the Journal of Hospital Medicine.
Performance Monitoring Systems
The VTE Collaborative worked with information technology experts to create a series of measures, such as the percentage of patients risk-stratified for VTE within 24 hours of admission and ordered risk-appropriate prophylaxis. Monthly reports were distributed to departmental leaders and quality improvement staff. The team also built an online database to assess performance at the level of institution, department, division, service and individual provider.
Provider-Level Dashboards and Pay-for-Performance
While computer-guided decision support improved risk-appropriate prophylaxis ordering to greater than 80 percent, additional measures are needed to approach 100 percent compliance. One step that has shown promise is the distribution of provider-level dashboards, allowing physicians to see their VTE prophylaxis ordering rates and compare them to other benchmarks. In a Johns Hopkins hospitalist service, monthly VTE prophylaxis compliance rates increased from 86 percent before introduction of web-based dashboards to 90 percent in their first month of use. The following month, the hospitalist service further incentivized VTE prophylaxis through an internal pay-for-performance program. After VTE measures were added to this dashboard, compliance reached 94 percent. This was published in a March 2015 Journal of Hospital Medicine article.
Tracking and Improving VTE Prophylaxis Administration
Even when appropriate VTE prophylaxis is ordered, there is no guarantee that patients will receive these treatments every time that they should. In a study, Johns Hopkins researchers discovered that nearly 12 percent of 103,000 ordered prophylaxis doses were not administered. This research, published in a June 2013 PLOS ONE article, and a follow-up study in the March 2014 Journal of Patient Safety also discovered that:
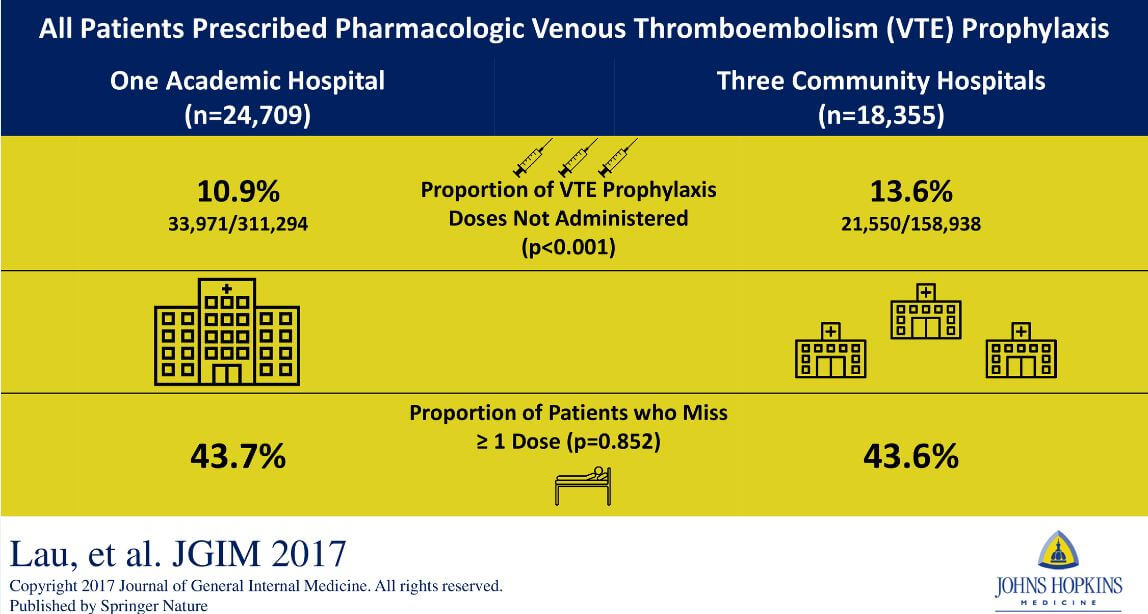
- Just 20 percent of patients who missed at least two ordered doses accounted for 80 percent of all missed doses.
- Nearly 60 percent of missed doses were due to the refusal of patients or family members.
- Nurses on low-performing units were more likely to agree that VTE prophylaxis is prescribed for patients who do not need it.
These findings support a strategy that targets a relatively small group of patients and clinicians for interventions, rather than a blanket approach, such as educating all patients.
Educating Nurses on Medication Administration Practice
As part of a multifaceted approach to improve VTE prophylaxis and directly addressing missed doses in an effort to decrease preventable harm from VTE, nurses were targeted to receive one of two online education modules. These web-based modules were assigned through a cluster randomized clinical trials and designed to educate nurses about the harms of VTE, benefits of VTE prophylaxis and strategies to better communicate this information to patients. This research published in an August 2017 PLOS ONE article found that:
- Overall nurse education reduced the frequency of VTE prophylaxis non-administration.
- Nurses found the interactive Dynamic module to be more engaging, enjoyable and enable better patient engagement.
These findings indicate that interactive, learner-centric education might be most appropriate to change practice and should be further applied to other domains of clinical education. Learn more at the Patient-Centered Outcomes Research Institute (PCORI) website.
Nurse education modules: Find this course, called "Venous Thromboembolism Prevention: The Nurse's Perspective," on the Armstrong Institute's learning management system. Johns Hopkins users can take it for free via myLearning.
A Patient-Centered Approach Improves VTE Prophylaxis Administration
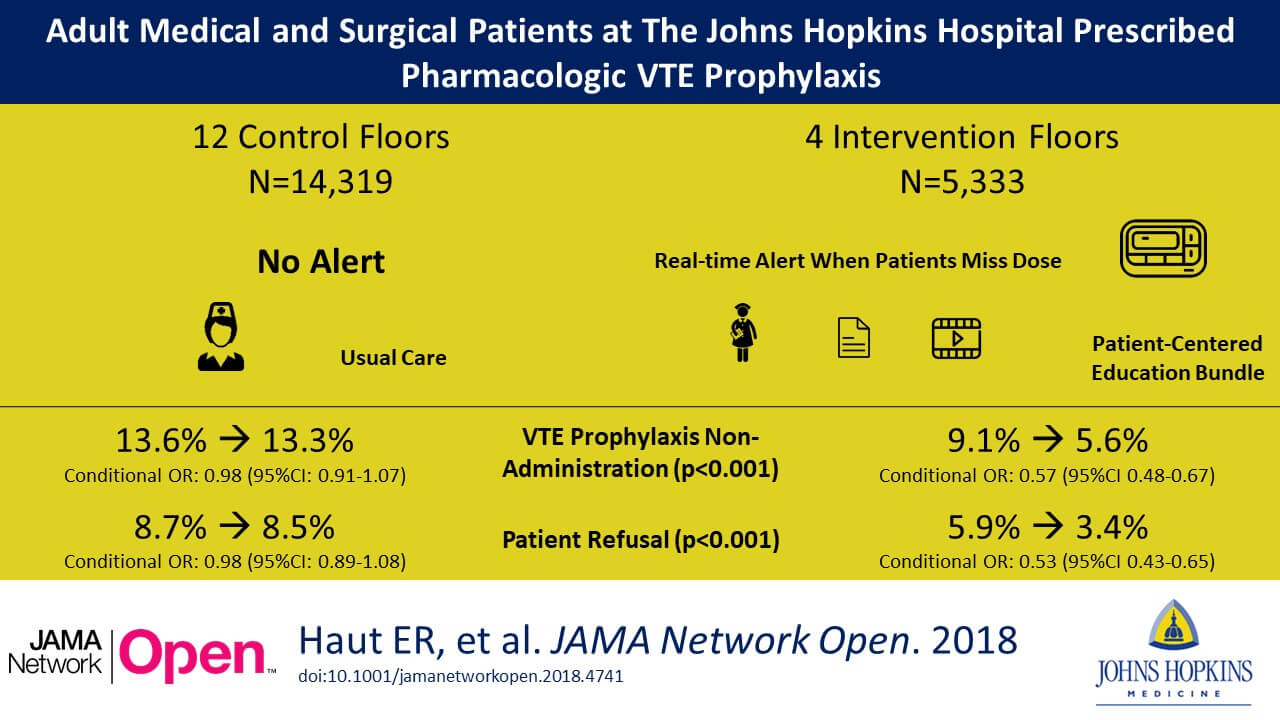
To improve VTE prophylaxis administration rates and reduce preventable VTE, an intervention was implemented that targeted patients who refused their pharmacologic VTE prophylaxis dose on medicine and surgery floors. During this intervention, we built an alert into our electronic health record (EHR) system, enabling our team to identify patients missing their VTE prophylaxis and to act on it in real time. We engaged these patients with the patient-centered education bundle (we previously developed) to help them to make an informed decision. This research is published in a November 2018 JAMA Network Open article, and found that:
- The intervention dramatically reduced the proportion of non-administered doses (43%) and of patient refused doses (47%) of VTE prophylaxis on intervention floors compared to control floors.
- These reductions in missed doses were associated with a 40% reduction in VTE events.
Our findings indicate that a targeted patient-centered education bundle improves health care quality by leveraging electronic data to target interventions in real time for at-risk patients.
Elements of a VTE Prevention Strategy
- VTE-prevention risk assessments must be a mandatory part of patient care
- Clinicians must identify VTE risk factors and contraindications to prophylaxis
- Clinicians must order risk-appropriate VTE prophylaxis
- Patient risk factors must be reassessed during their hospital stay
- The system must collect patient and provider data to monitor performance
- Adverse outcomes (e.g., hospital-acquired VTE and bleeding) must be monitored
- Performance must be measured regularly to promote continuous improvement