Hospital Readmissions
Patients are most at risk to return to the hospital immediately following discharge. Often new medication routines or lifestyle changes after being sent home can increase the chance of returning to the hospital. Access to community resources and family support can impact the chances that a patient returns to the hospital.
What is this measure?

Johns Hopkins Medicine hospitals track the number of patients with unplanned readmissions to the hospital within the 30 days after being discharged.
Readmission to the hospital could be for any cause, such as worsening of disease or new conditions. Unplanned hospital readmission is not always related to the previous visit.
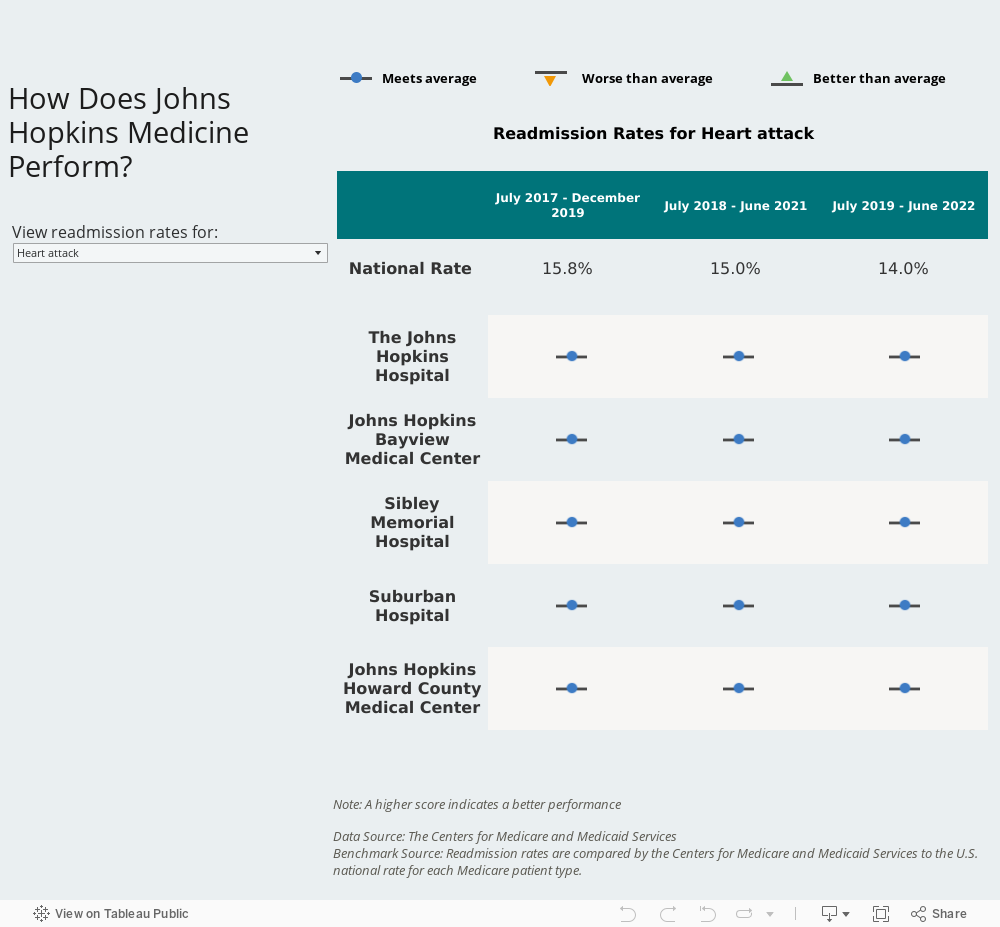
The Centers for Medicare and Medicaid Services (CMS) reports hospital readmission rates for Medicare patients who were admitted to the hospital for heart attack, heart failure, and pneumonia. CMS compares a hospital’s 30-day readmission rate to the national average for Medicare patients.
Why is it important?
Johns Hopkins Medicine hospitals track the number of patients with unplanned readmissions to the hospital within the 30 days after being discharged.
Readmission to the hospital could be for any cause, such as worsening of disease or new conditions. Unplanned hospital readmission is not always related to the previous visit.
The Centers for Medicare and Medicaid Services (CMS) reports hospital readmission rates for Medicare patients who were admitted to the hospital for heart attack, heart failure, and pneumonia. CMS compares a hospital’s 30-day readmission rate to the national average for Medicare patients.
What is Johns Hopkins Medicine doing to continue to improve?
Patients are most at risk for readmission right after discharge when they are often trying to follow new medication directions, making lifestyle changes, and managing follow-up appointments. Johns Hopkins Medicine attempts to fully prepare all patients before discharge and offers many programs for patients who need extra support after returning home.
Preparing for Discharge
Some Johns Hopkins Medicine hospitals have nurses called “transition guides.” Transition guides meet patients while in the hospital and then visit the patient at home for up to 30 days after discharge. These nurses ensure that patients are taking their medications correctly, answer any questions the patient may have, and review care instructions, like when to call the doctor.
Many Johns Hopkins hospitals have special pharmacy programs that provide bedside delivery for discharge medications. Pharmacists can visit patient rooms for extra instruction about high-risk conditions and the drugs used for treatment.
Helping with the Transition Home
Johns Hopkins Medicine has a Patient Access Line to support the care transitions of patients over the phone. Eligible patients receive a follow-up phone call from a nurse through the Patient Access Line within two days after being discharged from the hospital.
The nurse asks questions like:
- How is the patient feeling?
- Is the patient correctly taking their medications?
- Is the patient aware of their upcoming appointments?
The nurse then consults with the clinical team to address any concerns or find more resources.
Frontline Perspective
 Kathy Ward is the Manager of Case Management in the Department of Medicine at Johns Hopkins Bayview Medical Center. Her primary responsibility is to coordinate patients' services while they are hospitalized and the transition of care once they are discharged.
Kathy Ward is the Manager of Case Management in the Department of Medicine at Johns Hopkins Bayview Medical Center. Her primary responsibility is to coordinate patients' services while they are hospitalized and the transition of care once they are discharged.Kathy Ward, B.S.N., R.N., A.C.M., C.C.M.
Manager of Case Management, Johns Hopkins Bayview Medical Center
“The best part of my job is forming relationships with patients and their loved ones, and working with them to successfully transition the patient from the hospital to their home.
Patients who are discharged from the hospital are often at a high risk of being readmitted. This can be due to them having multiple health conditions, being uninsured, not having support systems in place or having a low level of literacy.
To make the patient’s transition plan from the hospital successful, I conduct a full medical, social and financial assessment, and coordinate with several key players, including home health services, financial counseling and community agencies.
I work to understand the motivations of my patients, educate them and, where needed, offer a ‘bundle of services’ for the highest-risk patients. I use data to understand how these different interventions can help reduce the risk of my patients being readmitted.
The one thing I will never do is ‘write a patient off.’ I love that I work as an advocate for my patients and can always customize or change and implement a new plan, if needed.”
How can patients and families support safety?
Understanding how to manage your health conditions is an important part of leaving the hospital. This includes knowing about any medications, dietary restrictions, or physical activity recommendations. Talk to your care team if you or a loved one have questions during the transition home or after discharge.