Physicians often detect early warning signs of dementia in their aging patients from the stories shared by a patient’s family members. They learn about situations that are out of character, such as paying a bill multiple times, misplacing keys and repeating stories. Often a patient has become more irritable and anxious.
When the clinical examination also suggests that a longtime patient’s behavior or disposition has changed, the next step is to rule out possible causes such as medication issues, poor sleep or traumatic life events, according to Esther Oh, co-director of the Johns Hopkins Memory and Alzheimer’s Treatment Center.
“When there’s clearly some functional impairment going on, I try to figure out why,” she says. “How older patients experience cognitive problems is complex.”
If physicians suspect a patient may have mild cognitive impairment due to Alzheimer’s disease or a related brain disease, they can order a variety of labs including blood tests, MRIs and CT scans, and may refer the patient to Oh and her colleagues in psychiatry, geriatrics or neurology at the Memory and Alzheimer’s Treatment Center.
There, patients can receive individualized treatment based on their needs, including medications targeting memory and cognition and treatments for mood, behavioral and sleep changes. Additionally, patients, caregivers and family members can get guidance and support that helps improve their quality of life, plan for the future and manage inevitable crises.
Much is still unknown about the disease. At this time, there’s no cure for Alzheimer’s, no proven way of slowing down its progression and no treatment available to reverse the deterioration that occurs in the brain.
Best practices for managing the disease include physical and social activity, healthy lifestyle and diet, and a well-structured environment. Older adults who engage in these behaviors appear to have less risk of cognitive and functional decline.
While the diagnosis is grim, Johns Hopkins clinicians and researchers are broadening Alzheimer’s and dementia research and expanding treatment options in a number of ways: searching for biological markers (biomarkers) that could predict Alzheimer’s; determining how to target certain proteins that are present in the brains of patients with the disease; defining the different kinds of Alzheimer’s to tailor future treatment and research; developing new drugs; and piloting a home-based care program.

Defining and Refining
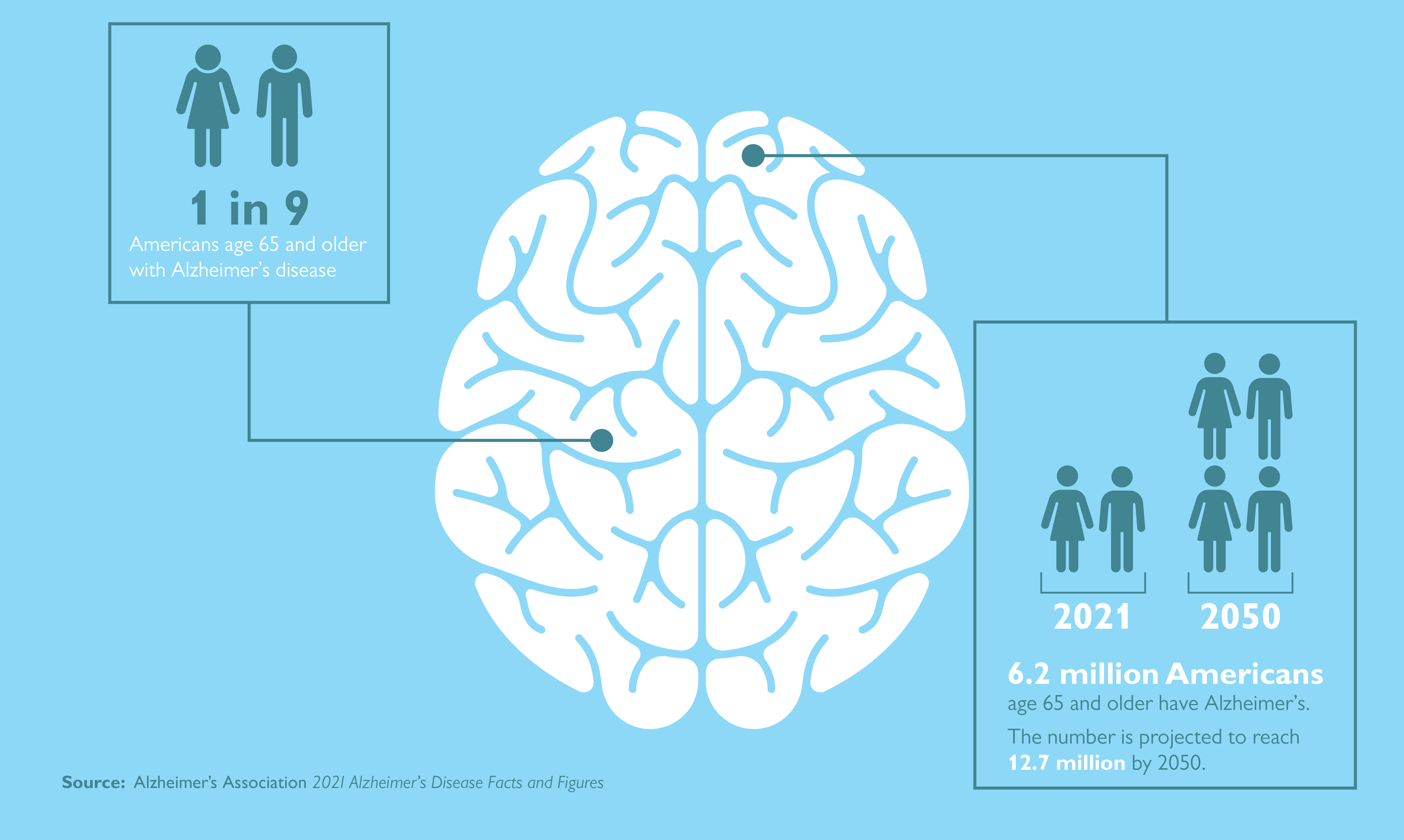
Dementia is a general term that refers to memory loss and decline of other cognitive abilities that limit independence in day-to-day function. Alzheimer’s is the most common brain disease that causes dementia among older adults, accounting for 60%–80% of cases. It affects an estimated one in nine people age 65 and older — 6.2 million Americans. This number is projected to grow to 12.7 million by 2050, according to the Alzheimer’s Association.
Almost two-thirds of the cases are in women, and people of color are at a higher risk of developing Alzheimer’s.
Alzheimer’s is a progressive, neurodegenerative disease that occurs when nerve cells in the brain die. It affects memory, thinking and behavior. But, unlike other forms of dementia, it does not affect patients’ motor function until late stages of the disease.
Alzheimer’s experts think individuals may experience different versions of the disease.
“It’s probably not one kind of Alzheimer’s disease, it’s probably many,” says psychiatrist Paul Rosenberg, co-director of the Johns Hopkins Memory and Alzheimer’s Treatment Center. “What we want to do is find the subtypes so we can find better treatments.”
Cancer treatment, for example, is specific to the kind and subtype of cancer. Breast cancer is treated differently from colon cancer, and within breast cancer, different subtypes mean different treatments. This is the direction in which Johns Hopkins researchers hope to move Alzheimer’s treatment.
Rosenberg and his colleagues, including Memory and Alzheimer’s Treatment Center director Kostas Lyketsos, are crunching data in the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease to do just that. The goal is to find characteristics that can allow physicians to predict which patients will develop Alzheimer’s, as well as determine what clinical data is necessary to differentiate subtypes of the disease.
The Precision Medicine Center’s patient registry includes more than 130,000 medical records that researchers hope can help define clinical subgroups of patients with dementia, determine when symptoms first develop and when diagnoses occur, among other factors. Additionally, center researchers are developing a collection of unique blood biomarkers that could help target future treatments to subgroups of patients.
Other projects include:
- Analyzing hundreds of MRIs from patients with dementia to look for variations in the size of different structures that could indicate subgroups.
- Studying changes in biomarkers over time to try to measure the progression of dementia.
- Using person-specific stem cells — which are made using a person’s own blood — to create different brain cells in the lab with the potential to predict response to specific medications that may have a role in improving cognitive decline.
- Treating brain vascular disease — an important contributor to dementia — by repurposing an existing drug, atorvastatin, which is typically used to lower cholesterol. Researchers are studying the drug’s effect on the brain’s circulatory system using a new MRI technique.
New Drugs in Development
Other Johns Hopkins researchers are testing a drug that has the potential to slow the progression of Alzheimer’s. Marilyn Albert, director of the Johns Hopkins Alzheimer’s Disease Research Center, Michela Gallagher, a professor of neuroscience at the Johns Hopkins University School of Medicine, and Arnold Bakker, director of the Johns Hopkins Psychiatric Neuroimaging Core, hope to receive FDA approval for the drug for patients in the earliest stages of the disease.
The drug targets two proteins: tau, which serves many functions in healthy neurons but can accumulate into tangles in cells, and amyloid, which forms plaques between cells. Gallagher theorized that periods of hyperactivity in the brain, such as seizures, push those proteins around the brain, spreading more tangles and plaques. She identified a compound, levetiracetam, that calms these hyperactive periods and is now approved by the FDA to treat seizures in patients with epilepsy when used with other medications. She and Albert are testing a time-release capsule version of levetiracetam taken at breakfast by patients in early stages of the disease.
The study, sponsored by AgeneBio, involves more than 164 people taking the drug for 78 weeks at 27 research sites across the country. Preliminary results are expected in fall 2022.
In addition to Albert and Gallagher’s drug, referred to as AGB101, there are more than 100 other Alzheimer’s drugs being tested at Johns Hopkins and elsewhere, according to the Alzheimer’s Association.
Universal Screening
As researchers wrestle with how to catch the disease in its early stages, the question of whether to do universal screening for cognitive impairment remains. Such screening is required as part of the Medicare Annual Wellness visit, initiated in 2011 as part of the Affordable Care Act. While primary care providers must perform this screening for Medicare patients, specialists at Johns Hopkins believe this kind of test can be useful in more targeted ways.
“There could be a place for targeted universal screening, but we have to be very careful,” Oh says. “The question remains, what are you going to do with that information?”
In some scenarios, screening may be appropriate, she says. For example, a patient undergoing surgery who has possible cognitive impairment could be screened in order to make sure they understand the procedure as well as post-op instructions. It could help providers manage possible complications, such as delirium after surgery, which occurs more commonly in individuals with dementia.
The Alzheimer’s Association recommends evaluation for people with memory concerns or cognitive complaints as well as for those with non-memory triggers, including personality change, depression, deterioration of chronic disease without explanation, and falls or balance issues. It is also recommended if a family member or loved one reports cognitive impairment.
Like Oh, Paul Rosenberg and Kostas Lyketsos don’t see a role for universal screening as there’s no demonstrated benefit from it.
“Until we have a safe and effective therapy that people can afford, it is just not ethical to do the tests,” Rosenberg says.