Brian Garibaldi remembers feeling a jolt of adrenaline tinged with fear when he saw the results. The patient, 61-year-old Liz Fox, had tested positive for the coronavirus that causes COVID-19.
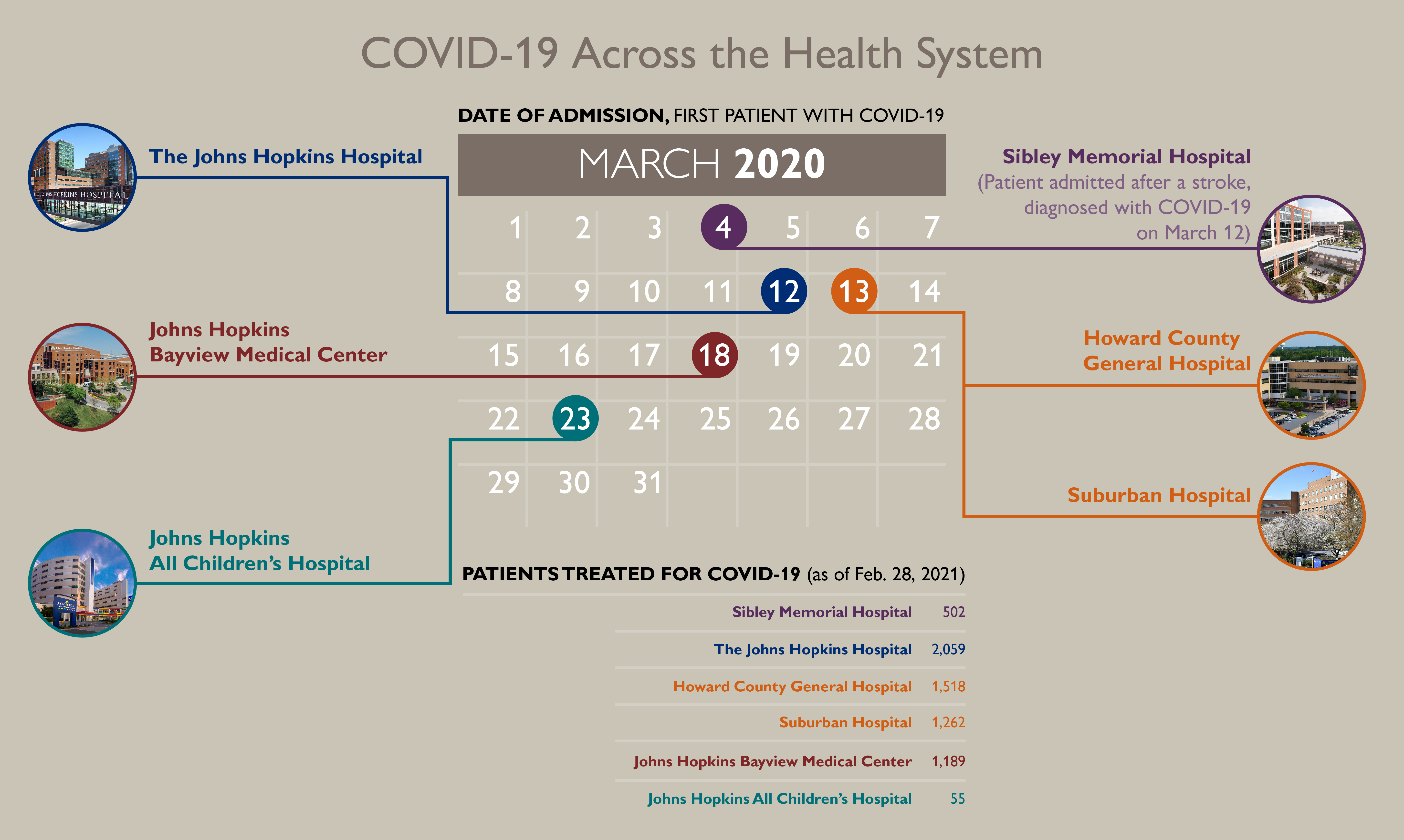
“It was a pretty scary time,” recalls Garibaldi, associate professor of pulmonary and critical care medicine and medical director of the Johns Hopkins biocontainment unit (BCU), where The Johns Hopkins Hospital treated its first patients with COVID-19.
“In addition to concerns about our own safety as providers, and the safety of our families and friends, we really had no idea what to expect clinically from these patients,” Garibaldi says. “We didn’t know the natural progression of this disease, how to interpret lab data or what treatments we could offer.”
Fox had arrived in the emergency department March 12, 2020, feeling so weak she could barely lift her cellphone.
“I was terrified,” she says of learning she had COVID-19. But she praises Timothy Niessen, the internal medicine doctor who provided care. “He told me not to be afraid,” she recalls.
Fox was treated in the BCU, never required ventilation and was released four days later. It took a few weeks to regain her strength, and she has felt fine ever since, she says.
“In those early days, I think we were all a little frightened — both patients and their doctors,” says Niessen. “There were no defined treatments, and our research programs weren’t up and running yet. The people in the room, even in those loud and bulky air purifying respirators, had a huge role in reassuring our patients that whatever comes, we’d confront it together.”
By Feb. 28, 2021, the health system’s six hospitals had treated 6,584 patients for COVID-19, including 1,838 who were discharged after receiving care in intensive care units, and 643 who died.
The number of Johns Hopkins Medicine (JHM) patients who had tested positive for the coronavirus that causes COVID-19 was 19,397.
Like an enormous tidal wave crashing into Johns Hopkins Medicine, the deadly coronavirus has pushed waves of change into every corner of the organization.
The institution emerging from the pandemic is, in many ways, stronger. It offers greater flexibility for patients and employees, it remains committed to delivering better care to its neighbors, and it is more prepared for the next crisis.
It is also better equipped to handle the current crisis. Clinicians throughout the health system know a lot more about how the virus that causes COVID-19 spreads and responds to treatment.
They now know, for example, that they can safely care for patients without jeopardizing their own health or infecting their loved ones.
They know that older patients are more likely than young ones to get severely ill or die from COVID-19, and that the risk increases if SARS-CoV-2 infects a person with conditions such as obesity, diabetes, hypertension and cancer. They know that Black, Latinx and Native American people face disproportionate risks from the coronavirus.
They know that high-flow oxygen is often better for patients than invasive mechanical ventilation, and that putting very sick patients on their stomachs can improve breathing. They are learning which medications work, and when they are most effective.
It has been a long, awful year, suffused with human loss and suffering almost beyond comprehension.
“It’s been so incredibly tragic and challenging,” says Lisa Maragakis, senior director of infection prevention for the health system. “And we’re not out of it yet.”
But hope warms these late-winter days, as more people get vaccines, COVID-19 hospitalizations drop, and clinicians and researchers keep learning about the virus.
Capturing Our Resilience in Poetry

Mia Scharper, a Johns Hopkins Medicine International employee, delivers “March,” a moving poem she wrote about employees’ resilience during the COVID-19 pandemic and their hope and healing moving forward. She is accompanied by Peabody Institute cellist Lindsey Choung.
A Changed Landscape
The institution responded to a terrifying and little understood global health crisis by doing what it does best: treating patients, protecting staff members, marshaling its vast research apparatus, supporting its communities, and providing crucial and clear-eyed information to a world desperately hungry for facts.
“Johns Hopkins Medicine is built upon a legacy of service,” says Kevin W. Sowers, president of the Johns Hopkins Health System and executive vice president of Johns Hopkins Medicine. “Our organization was created to support a greater good, to help the world navigate some of the toughest challenges humanity will ever face. We were made to respond to moments like this one.
“At its core, JHM is an organization made up of compassionate, intelligent, driven individuals who live our mission every day. I’m so very proud of the people of JHM for taking care of our patients, supporting our communities, caring for one another and continuing to move our mission forward even in the face of the greatest public health crisis of modern times.”
The following are some of the ways COVID-19 has changed how Johns Hopkins Medicine cares for patients, employees and the community. (Click here to read about JHM's member organizations and the school of medicine.)
Hospital Epidemiology and Infection Control (HEIC): Infection prevention teams across Johns Hopkins Medicine have been leading the institutional response to COVID-19 since early January 2020. They set up an HEIC incident command center to prepare and plan, to obtain supplies such as N95 respirators, and to create new infection prevention policies, protocols, communications and procedures for the safe identification and care of patients with COVID-19.
The infection prevention teams, in collaboration with facilities, nursing and other departments, worked with institutional leadership to develop and implement a strategy throughout Johns Hopkins Medicine for patient placement.
When doctors, nurses and other clinicians moved from their usual assignments to COVID-19 care, they had to learn new skills, including how to put on and take off cumbersome personal protective equipment (PPE).
“We set up a safety officer program to teach and support our policies, and to monitor and assist in the COVID-19 units and other areas to make sure people are safe, wearing the right PPE, and protecting themselves and others,” says Maragakis.
JHM Unified Incident Command Center: Starting in January 2020, the Johns Hopkins Office of Critical Event Preparedness and Response (CEPAR), the Johns Hopkins Medicine Office of Emergency Management, HEIC infection control teams and key Johns Hopkins Medicine individuals began tracking the novel coronavirus and developing a plan for the health system. On March 3, they launched the JHM Unified Incident Command Center in the Chevy Chase Auditorium.
In a March 10, 2020, podcast for the Johns Hopkins Bloomberg School of Public Health, Gabor Kelen, CEPAR’s director and a professor of emergency medicine, outlined some of the questions the command center was considering: “Where are we going to put patients, and in what order? How do we screen patients? What are the implications for our workforce policies related to travel, self-monitoring and return to the clinical area? What are the best practices for use of personal protective equipment?”
Every day, members of the JHM Unified Incident Command Center identified the top problems and set out to find solutions. One group developed infection control protocols, another led creation of a call center to answer employee questions, a third determined best practices for collecting and analyzing test results and other patient information.
“I think our pandemic response has really accelerated our progress toward acting as one organization,” Maragakis says.
Download text-only version: Word | PDF
Facilities: As the first patients with COVID-19 arrived, facilities department teams across the health system modified the air handling and physical structure of entire floors of Johns Hopkins Medicine hospitals to help turn them into isolation units for the safe care of patients with COVID-19.
They constructed spaces for putting on and taking off PPE, and altered the heating, ventilating and air conditioning systems so that rooms had negative air pressure to contain the virus.
Now, with notice, portions of the hospitals can be switched back and forth from COVID-19 care to non-COVID-19 care areas, as needed.
Supply Chain: Global shortages of PPE and other supplies created some of the biggest challenges in the pandemic’s early days, when the virus caused both a spike in demand and a drop in manufacturing.
The supply chain team was able to overcome enormous challenges and barriers to procure the necessary supplies, including N95 respirators and other critical items, in a complex global market. They were innovative, even acquiring equipment from unconventional sources such as a car manufacturer that made reusable isolation gowns from air bag material.
“We never ran out of any critical supply, knock on wood,” says Burton Fuller, health system vice president and chief supply chain officer. “The pandemic forced us to start acting and functioning like one health system. It will be easier for us to accommodate supply disruptions in the future.”
Patient and Family-Centered Care: One of the most heartbreaking aspects of COVID-19 has been the restrictions on visitors accompanying patients into hospitals and clinics. “We feel so strongly about the value of having a care partner at your side,” says Lisa Allen, chief patient experience officer.
The health system responded by making sure loved ones stayed connected and informed. Patients have access to cellphones, chargers, and hospital iPads equipped with Zoom. Now, says Allen, “The health care teams are trying to make sure families are updated with phone calls at least once a day.”
The visitor limits, plus widespread use of face masks and air-purifying respirators, have made communication between patient and provider more difficult, especially for patients who are not fluent in English.
Tina Tolson, senior director of operations for Johns Hopkins Medicine Language Services, says the pandemic accelerated efforts to centralize patient communication services across the system, and to expand audio and video interpretation — typically, access to over 200 languages is available in less than a minute.
Tools to promote effective communication with patients have been even more critical than usual during the pandemic, with in-person interpreters limited in order to minimize spread of the virus.
Telemedicine: When nonemergency surgeries and routine appointments were restricted, the health system dramatically increased its telemedicine offerings. “Almost overnight, we transitioned how we deliver care,” says Brian Hasselfeld, medical director for digital health and telemedicine.
Remote video and telephone doctor appointments skyrocketed from about 60 per month in February 2020 to nearly 90,000 in May, with psychiatry, family care, neurology, and preop and postop neurosurgery appointments among the most popular telemedicine categories.
The number has since dropped to about 55,000 per month as patients returned to in-person appointments, but Hasselfeld notes that is nearly 1,000 times higher than before the pandemic. Citing strong patient satisfaction scores, he expects telemedicine to remain a convenient option for clinicians and patients.
Community Support: The health system and The Johns Hopkins University responded to need by creating the multipronged COVID-19 Pandemic Anchor Strategy, which brought COVID-19 information, testing and resources to underserved populations, including in nursing homes and homeless shelters.
“As a health system, we recognized that in order to reach the most vulnerable communities, we had to bring COVID-19 testing to them,” says Sherita Golden, vice president and chief diversity officer for Johns Hopkins Medicine.
In collaboration with BUILD (Baltimoreans United in Leadership Development), Johns Hopkins Medicine established a mobile COVID-19 coronavirus testing site at the Sacred Heart of Jesus church in the Highlandtown neighborhood of Baltimore. People also had access to food delivery at the testing site, and referral to the Lord Baltimore Hotel for COVID-19 isolation and recovery.
Meanwhile, the East Baltimore COVID-19 Food Access Initiative, created by Johns Hopkins and community partners, has delivered 4.6 million meals to Baltimore families.
The focus now is on making sure that all marginalized populations have access to COVID-19 vaccines, says Golden. In partnership with Baltimore City and Washington, D.C., health care systems including Johns Hopkins Medicine are setting up vaccine clinics to reach people with less access and fewer opportunities for vaccination.
“We have established vaccine equity and outreach programs for our nonclinical front-line employees, patients without active MyChart accounts and patients seen in our clinics that care for the underserved,” she says.
Tapped by the state of Maryland, Johns Hopkins Medicine is also vaccinating public school teachers in Baltimore City and in Howard and Montgomery counties, and has created community vaccination programs in Montgomery County, including at Suburban Hospital.
Employee Support: Early in the pandemic, expansion of the peer support program RISE (Resilience in Stressful Events) helped clinicians cope with the stress and trauma brought on by COVID-19.
The Office of Well-Being facilitated coordination of a multilayered support system that includes wellness, psychiatry and spiritual resources. “I remember thinking it’s great that our front-line workers and leaders are taking care of us, but who is taking care of them?” says Lee Daugherty Biddison, chief wellness officer for Johns Hopkins Medicine. She expects the services to remain for employees after the pandemic recedes.
Recognizing that the pandemic also brought financial strains, Johns Hopkins established meal and grocery pick-up sites for employees, and created the Emergency Assistance Support for Employees (EASE) Fund to help with medical expenses, child care and other costs associated with COVID-19.
In mid-March 2020, thousands of nonclinical employees abruptly switched to remote work. In January of that year, 2,600 Johns Hopkins Health System employees — about 9% — were working from home. A year later, 8,500 employees, or 27%, are working remotely.
“It was a scramble at the start,” says Inez Stewart, senior vice president, human resources, Johns Hopkins Medicine. “We had to very quickly put some processes and tools in place to make sure people are connected and productive.” She expects some flexibility about working remotely to remain.
Learning As They Go
Most Johns Hopkins research labs closed in March 2020 then reopened in May with limits on how many people could be there at one time. Many investigators found new purpose as part of a high-stakes global race to understand the novel coronavirus.
In the pandemic’s earliest days, when COVID-19 screening tests were both scarce and slow, Johns Hopkins clinical microbiologists Karen Carroll and Heba Mostafa created an in-house version of the test.
Johns Hopkins was one of the first institutions in the state to provide its own testing. The Johns Hopkins microbiology laboratory now uses 11 platforms to analyze about 2,500 COVID-19 coronavirus tests per day — including a rapid point-of-care test — for people with and without symptoms. A test that uses saliva, developed in November 2020, by a team at the Johns Hopkins molecular pathology laboratory, has a current capacity of 4,000 tests per day for screening health care workers and undergraduate students.
In recent months, Mostafa’s research lab began sequencing the virus, and it can now identify variants that might respond differently to vaccinations or treatment. Her lab was the first, in January 2021, to report a South African variant in Maryland.
Like other Johns Hopkins researchers, Mostafa is learning about the virus as she goes.
Physician Brian Garibaldi, with biostatistics professor Scott Zeger and others, established JH-CROWN, a database of COVID-19 patient information and biological samples to be used by the new Johns Hopkins Precision Medicine Center of Excellence for COVID-19. Like others at Johns Hopkins, this precision medicine center uses large amounts of data to research how individual patients are likely to respond to disease and treatment.
In addition to publishing a COVID-19 inpatient risk calculator that is now available for front-line clinicians, the Precision Medicine Center of Excellence for COVID-19 added a prediction model to the Epic medical record system. This model, created by infectious disease specialist Matthew Robinson and medical student Shannon Wongvibulsin, uses patient symptoms and demographic data to determine if a hospitalized patient will progress to severe illness or death.
“We now know how to approach not just the care of patients, but how to learn from patients,” says Garibaldi.
Daniel Ford, director of the Johns Hopkins Institute for Clinical and Translational Research, has recruited more than 11,000 people who have tested positive for the COVID-19 coronavirus for possible participation in clinical research. His group is making sure to recruit people of color in order to create studies that include and benefit everyone.
“We have about 35 different therapeutic trials set up for COVID,” says Ford. “Just for clinical studies, there are 50–75 people who are working on COVID.”
One such researcher is Shmuel Shoham, an infectious disease specialist. Between 2012 and 2015, he studied the role of convalescent plasma to treat influenza, and he wondered if the therapy could help people with COVID-19.
The resulting National COVID-19 Convalescent Plasma Project, chaired by Johns Hopkins immunologist Arturo Casadevall, is looking at whether the antibody-rich blood of people who survive COVID-19 can be used to treat others with the disease. Interim results are expected soon, says Shoham.
Paul Auwaerter, clinical director of the Johns Hopkins Division of Infectious Diseases, leads a group of about 100 Johns Hopkins experts in infectious diseases, pulmonary and critical care medicine, clinical pharmacology and pharmacy who review the latest COVID-19 science and distill it for Johns Hopkins care providers.
The group’s first guidance, released March 25, 2020, notes: “At the time of this writing, there is minimal available evidence from randomized clinical trials to support recommendations for the use of any specific pharmacologic treatment for patients with COVID-19.”
Less than a year later, in February 2021, the recommendations included nuanced assessments of when to use remdesivir, dexamethasone, convalescent plasma and monoclonal antibodies.
Emerging Stronger
On a February night, Garibaldi, the pulmonologist and biocontainment unit medical director, reflected on the past year as he drove home from a shift treating patients with COVID-19. With hospitalizations dropping, he had been transitioning part of a medical intensive care unit back to non-COVID-19 care.
“I hope this is a sign of more days like this to come, when we can decommission more units,” he says.
Garibaldi notes that the health system can now respond quickly to ebbs and flows in the number of patients with COVID-19. “We have much more capability to handle a surge in COVID patients than we did in April,” he says.
And more confidence, too.
“There was a lot of uncertainty back in March of 2020 in terms of what caring for these patients would truly be like,” says Garibaldi. “It’s easy to forget how concerned we all were for the safety of our health care workers, our families and our communities.
“Back then, even though only a few people were in the room with those first COVID patients, it was an institutionwide response. That’s still true.”