
Esophageal Manometry
If the muscles in your esophagus, the tube that connects the mouth with the stomach, don’t function properly, your doctor might recommend esophageal manometry to test why this is happening.
What is esophageal manometry?
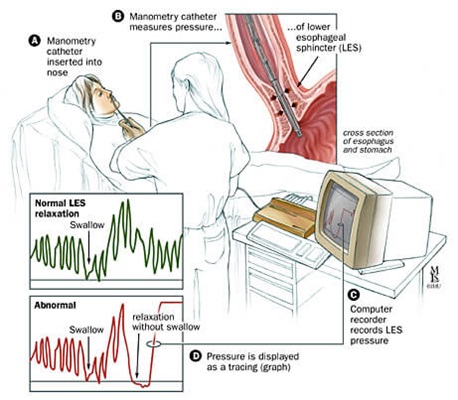
Esophageal manometry is a test that examines the coordinated muscle movement (motility) of the esophagus. The test uses a narrow, flexible, pressure-sensitive tube called a catheter. The catheter measures pressure created by the muscles in the esophagus and the valves in the top and bottom portions of the esophagus. These valves, called the upper and lower esophageal sphincters, control how food enters and exits the esophagus.
High Resolution Esophageal Manometry
High resolution esophageal manometry is a version of the test that uses a catheter that has many more sensors than a traditional catheter. The sensors are also closer together. The greater number of sensors means that high resolution esophageal manometry can collect more data and collect it faster than a traditional procedure.
Who may need esophageal manometry?
Esophageal manometry is used to check whether the muscles in the esophagus are working properly. When the muscles don’t work as they should, you may experience symptoms such as heartburn, trouble or pain when swallowing, chest pain and regurgitation (food coming back up after swallowing). Esophageal manometry helps determine what is causing these symptoms, which could be conditions such as:
- Achalasia (esophagus muscles don’t help move food down and prevent food from entering the stomach)
- Diffuse esophageal spasm (esophagus muscles contract randomly and interfere with swallowing)
- Scleroderma (a rare disease that may cause some esophagus muscles to stop moving)
Esophageal manometry can also be performed in preparation for esophageal surgery or to follow up and assess function after surgery.
Esophageal Manometry with Impedance
Esophageal manometry can also be used before an esophageal pH (impedance) test, which helps diagnose gastroesophageal reflux disease (GERD). Combined, these tests are called esophageal manometry with impedance. The pH test measures the presence of acids and other digestive fluids in the esophagus. Manometry helps determine where in the esophagus to place the pH probe.
Esophageal Manometry Versus a Barium Swallow
Both esophageal manometry and barium swallow studies are used to evaluate trouble swallowing and related symptoms. Barium swallow involves drinking a thick solution containing barium, which is a contrast agent — it shows up on an X-ray. It can help spot abnormally wide or narrow areas of the esophagus, as well as abnormalities in the anatomy, which esophageal manometry doesn’t do.
The manometry test senses the pressure and constriction of muscles in the esophagus as you swallow. It can detect patterns of muscle activity throughout the length of the esophagus, including contractions that are too weak or too powerful. A barium swallow study can’t measure the strength of muscle contractions.
Based on your symptoms, your doctor may recommend one or both of these tests.
Preparing for Esophageal Manometry
Your gastroenterologist will provide specific instructions to follow before the procedure. Typically, eating and drinking must be avoided for at least six hours before the test. Be sure to tell your doctor about any medications and supplements you take. Your doctor will let you know if you need to change when and how you take them the day before or the day of esophageal manometry. (If you have diabetes, skipping breakfast may affect your need for medication.)
What happens during esophageal manometry?
Esophageal manometry is usually an outpatient procedure, meaning you can go home the same day. The test lasts about 30–45 minutes and can be performed by a nurse practitioner or another trained health care provider.
During an esophageal manometry:
- You sit in an upright position as a nurse applies a numbing gel to one of your nostrils and a numbing spray to the back of your throat.
- The nurse guides a narrow catheter through the numbed nostril into the throat while you swallow. The catheter is advanced through the esophagus as you continue swallowing, until it reaches the stomach. Your eyes may water and you may gag as the catheter is advanced, but you should not feel pain.
- Once the catheter is in place, the table is reclined so that you are lying on your back. You will be able to breathe and talk.
- To take a benchmark pressure reading, you will be asked not to swallow for 30 seconds.
- You will take sips of varying amounts of water at intervals as instructed. At one point, you may be asked to gulp water as fast as you can. If you are having esophageal manometry with impedance, you’ll sip a saline solution instead of water to help measure pH levels. You may be asked to sit up during parts of the test.
- If you have trouble swallowing certain foods, the nurse may ask you to swallow them during the test to see what could be wrong.
- The catheter’s pressure sensors measure how your esophagus muscles contract and relax as you swallow. The sensors send information to a computer that records your swallowing patterns for a doctor to analyze. The nurse may move the catheter slowly to measure pressure in different parts of the esophagus.
- When the test is over, the catheter will be removed slowly. You can return to your normal activities immediately after the test.
Esophageal Manometry Test Results
A few days after the procedure, your doctor will contact you to discuss the test and what the results reveal about the muscle function in the esophagus. Interpretation of esophageal manometry results takes specialized skill, and sometimes the results do not point to a definite cause of the symptoms. A normal esophageal manometry may call for more diagnostic tests.
Risks and Side Effects of Esophageal Manometry
Esophageal manometry is generally a safe procedure. Serious problems are extremely rare, but include:
- Arrhythmia (irregular heartbeat)
- Aspiration (inhalation of stomach contents)
- Esophagus perforation (the tube penetrates the wall)
- While the tube is being positioned, it may enter the larynx (voice box) and cause a choking sensation, which your motility nurse will address right away by adjusting the tube.
After the procedure, you may experience:
- A sore throat, which can be relieved with over-the-counter throat lozenges
- Temporary congestion in your nose
- Minor nosebleed



