Vasectomy Reversal
How often do men seek vasectomy reversal? Why?
Approximately 6 percent of all men who undergo vasectomy will later desire reversal. Often it is because they have a new partner, while in many cases the couple has simply decided that they would like more children. Additionally, chronic scrotal pain can develop in 1 – 2 percent of men who undergo vasectomy, often requiring a vasectomy reversal to alleviate the pain.
How should I choose where to get a vasectomy reversal?
While many clinics offer and advertise vasectomy reversal, it is important to consider that the success of the operation is heavily dependent on the surgeon’s training, experience, surgical precision, intraoperative decision-making skills, state-of-the-art equipment and support team. Fellowship training is extremely important to obtain excellent patency and pregnancy rates.
Where are sperm made, and what is their normal path?
Sperm production occurs in the testis at a rate of 60 million sperm per day per testicle. From the testes, sperm travel to the epididymis. The epididymis is a continuous, tightly coiled tube approximately 15 – 18 feet in length, which leads into the vas deferens. In the epididymis, the sperm mature and develop motility. Thus, sperm that have not passed through the epididymis are generally not able to fertilize eggs under normal conditions. The vas deferens is responsible for directing and propelling sperm into the urethra, where it joins with fluid from other glands to form the ejaculate.
What happens during a vasectomy?
During a vasectomy, the vas deferens (the tube that carries sperm into the ejaculate) is divided or interrupted by one of many methods, including removal of a tube segment, placement of clips on the vas or using electric energy to cause scarring and closure of the tube.
What is done during a vasectomy reversal procedure?
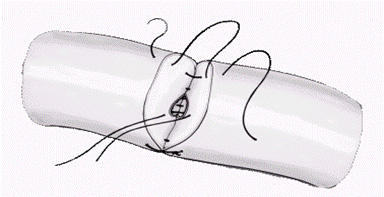
Vasectomy reversal reestablishes an open tube, or “lumen,” of the vas deferens to allow the sperm to reach the ejaculate once again.
To accomplish this, the vas deferens is connected to a healthy segment of vas deferens (vasovasostomy) or to a tubule of the epididymis (vasoepididymostomy).
Which is preferred, vasovasostomy or vasoepididymostomy?
The path lumen within the vas deferens is around one-third of a millimeter in diameter. The lumen of the epididymis can be one-third to one-half of this size. Thus, when possible, vasovasostomy is preferred.
Why would a surgeon perform vasoepididymostomy?
The decision of whether to perform a vasovasostomy or a vasoepididymostomy depends upon the quality of the fluid from the vas deferens at the time of surgery, patient characteristics such as time since vasectomy (greater than 10 years) and surgeon experience. Sometimes the sperm can be blocked in a region separate from the vasectomy site — often in the epididymis after a prolonged time since vasectomy. In these cases, bypassing the vasectomy site with vasovasostomy will not suffice to allow sperm to reach the ejaculate. Using intraoperative findings, an experienced surgeon will be able to decide the appropriate procedure. Since this decision is made during the surgery, it is important to have a surgeon who is experienced, confident and prepared for either operation.
How do some clinics perform vasectomy reversal with very low cost?
Using suboptimal magnification equipment can drastically cut the cost of the procedure. However, optimal magnification has been shown to improve outcomes. In addition, when a proper surgical microscope is used, general anesthesia is usually preferred. However, many clinics using lesser magnification will perform the operation under local anesthesia to cut costs. Others cut costs by performing only vasovasostomy to limit the time of the operation, even when vasoepididymostomy would be preferred by an experienced surgeon. Finally, using optimal suture adds to the cost of the procedure; the suture used is practically invisible to the naked eye, and it’s critical to the success of the operation.
How is vasoepididymostomy performed?
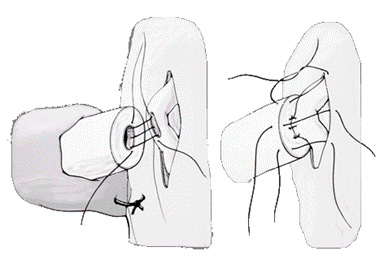
Vasoepididymostomy (or epididymovasostomy) requires even more experience and surgical precision for optimal results. As mentioned, the decision to perform vasoepididymostomy is made during the operation, so it is imperative that the surgeon is prepared and experienced in this technique.
To perform vasoepididymostomy, a single epididymal tubule is carefully dissected and mobilized. It is then incised in a location upstream from the suspected obstruction. The fluid is checked for sperm and, if none are present, another transection is made closer to the beginning of the epididymal tubules. The anastomosis (connection) is then performed with two layers of extremely fine suture under the operating microscope.
What should I expect on the day of vasectomy reversal surgery?
You will be asked not to eat or drink anything the night before surgery, as a measure to decrease the chance of complications with anesthesia. You will then present to the facility and meet with the anesthesia team and doctor. The procedure is done under general anesthesia, meaning the patient is completely asleep. It is an outpatient surgery, so patients return home or to a nearby hotel without actually being admitted directly to the hospital. This saves considerable expense and makes the overall experience much more pleasant.
How long does the vasectomy reversal surgery take?
Vasovasostomy or epididymovasostomy usually takes approximately 2.5 – 4 hours, although it can be significantly longer in certain cases.
What is the vasectomy reversal recovery process?
Postoperative follow-up includes an evaluation of the healing wound at 2-3 weeks, although many foreign patients forego this visit for convenience purposes.
When do you check for success after vasectomy reversal?
Semen analysis is usually first checked between two and three months after surgery. Semen analyses are then obtained for approximately 4 – 6 months, or until the sperm count stabilizes. It can take up to 6 – 12 months for sperm to return to the ejaculate following a vasovasostomy and longer following an epididymovasostomy (up to 18 months). However, in the vast majority of patients, sperm will be seen in the ejaculate three months after vasovasostomy. If semen quality is less than expected, anti-inflammatory medications may be prescribed to decrease scar formation that can block the surgery site.
Are there alternatives to vasectomy reversal?
Adoption and the use of donor sperm with assisted reproductive techniques (ART) are entirely acceptable options. If a man does not want vasectomy reversal, testicular or epididymal sperm extraction can be used to obtain sperm for IVF or ICSI. In many cases, depending on the female partner’s age, ART might be advisable instead of natural conception. In this case, sperm retrieval might make more sense for the couple than vasectomy reversal.
What backup approaches are available in case the vasectomy reversal is not successful?
Cryopreservation of sperm (sperm banking) can be performed at the time of vasectomy reversal. Sperm can be acquired by testicular sperm extraction (TESE) in most patients, and from epididymal or vasal fluid in some patients.
Because vasectomy reversals may infrequently scar over time despite good initial results, cryopreservation may also be performed on ejaculated specimens early in the course of recovery. However, since most couples are hoping to conceive naturally, and since the surgery is usually successful, most couples choose to later pursue TESE only if necessary.



