Tele-Dizzy Consultation and Trial Opportunities for External Health Sites
Demonstrated Clinical Need
Diagnostic Errors and Harms: A Public Health Crisis
- Diagnostic errors lead to an estimated 800,000 permanent disabilities and deaths in America each year (Newman-Toker et al., 2024).
- The estimated costs of these disabilities and deaths to US society are $200 billion to $1 trillion per year (Newman-Toker et al., 2018).
- Annual US healthcare waste associated with these errors is probably $50-100 billion or more (Natarajan et al, 2021; Newman-Toker et al., 2013; Schwartz et al., 2012; Smith et al., 2013).
The Stroke Imperative
- Stroke is the number one cause of serious misdiagnosis-related harms, affecting roughly 100,000 per year (Newman-Toker et al., 2024).
- Stroke is also the top cause of malpractice payouts in the emergency department (ED) (Newman-Toker et al., 2022).
- Strokes are not missed in the ED when they are obvious; they are missed when they are subtle or atypical (Newman-Toker et al., 2022). The number one risk factor for missing a stroke diagnosis is a clinical presentation with dizziness or vertigo (Tarnutzer et al., 2017).
The Dizziness Imperative
- Dizziness affects 15-20% of adults each year (Neuhauser, 2016) and leads to nearly 5 million ED visits annually (Badihian et al., 2020).
- Length of stay (Kerber et al., 2010) and costs of care (Saber Tehrani, 2013) are disproportionately higher in dizziness, but much of this is waste (Newman-Toker et al., 2013).
- Best evidence-supported (Fife et al., 2008; Tarnutzer et al., 2023) and guideline-supported (Edlow et al., 2023) bedside diagnostic care for ED dizziness is rarely applied (Kerber & Newman-Toker, 2015).
Overview: Tele-Dizzy Consultation Concept
Portable video-oculography (VOG) is a technology that facilitates remote video interpretation of bedside eye findings by expert neuro-vestibular consulting physicians. Our goal is to use VOG-enabled teleconsultation to improve diagnostic accuracy, health outcomes, and ED workflow for patients presenting with acute dizziness who lack any obvious acute stroke symptoms. The consultation is based on evidence-based eye movement exams proven to be more accurate than MRI scans (Tarnutzer et al., 2023). After excluding clear “brain attack” suspects (e.g., weakness, speech problems), ED patients with dizziness or vertigo are referred for remote consultation to help distinguish common inner ear diseases from dangerous strokes that can result in serious patient harms (Society to Improve Diagnosis in Medicine, 2020) and major malpractice lawsuits (Associated Press, 2006).
The consultation begins when local personnel record a 10-15–minute eye movement test battery using an FDA-approved, portable video-oculography (VOG) device (ICS Impulse, 2015). Recordings are sent digitally (asynchronously, in near real-time) to a Johns Hopkins vestibular neurologist. Within an hour, the consultant neurologist recommends a diagnosis and management plan to the ED team (Figure 1). As needed, the vestibular specialist interacts directly with either the physician or patient.
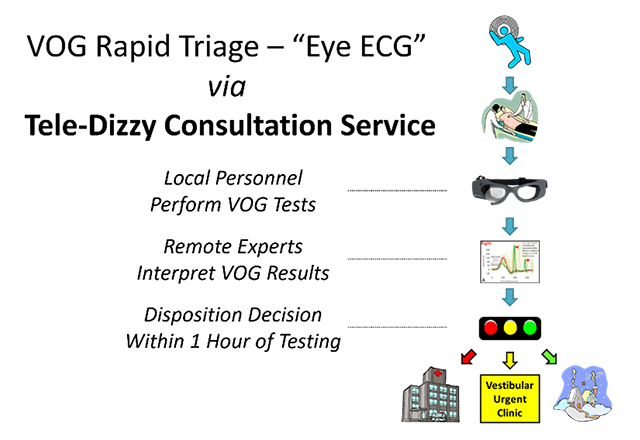 Figure 1. Overview of Tele-Dizzy consultation concept. Abbreviations: ECG, electrocardiogram; VOG, video-oculography.
Figure 1. Overview of Tele-Dizzy consultation concept. Abbreviations: ECG, electrocardiogram; VOG, video-oculography.
What is the process to implement Tele-Dizzy at a new institution?
The main thing your ED will need to do is provide a workforce of technicians (or nurses, physicians assistants, etc.) who will perform VOG testing. This means local “champions” (superusers) will be trained and help maintain this local workforce. Our Johns Hopkins team will help provide the initial training for your champions (roughly two half days) plus feedback on their first 10 cases (for assessment of competence and quality assurance for these superusers).
Overall, there are several logistical work streams essential to the clinical deployment:
- Equipment procurement and information technology clearance/integration
- Technician “champion” training on VOG equipment and eye movement test battery
- Johns Hopkins physician licensure, credentialing, and provider enrollment
- Clinical services and related legal agreements with Johns Hopkins
- Outcomes and analysis plan to assess impact of service delivery
Each aspect will be tailored to your local context. These work streams will all be completed in partnership between your local team and the Johns Hopkins Tele-Dizzy implementation team. They take approximately 6 months to complete.
VERTIGO Trial vs. Tele-Dizzy
Summary of key differences and similarities between the VERTIGO trial and Tele-Dizzy.
The proposed V.E.R.T.I.G.O. Trial (Vestibular Emergency Room Teleconsults vs. Imaging for better diaGnostic Outcomes) compares video-oculography (VOG)-enabled teleconsults to a neuroimaging-first strategy to improve diagnosis of stroke vs. inner ear disease and associated health outcomes for adult ED dizzy patients. The main differences between VERTIGO and Tele-Dizzy are that VERTIGO randomizes the timing of implementing Tele-Dizzy, patient eligibility is more tightly managed, and structured data need to be captured in follow-up.
| Parameter | VERTIGO Trial to Study Tele-Dizzy | Clinical Tele-Dizzy Service |
|---|---|---|
| Overall Program Type | Hybrid Research (clinical trials) & Operations (clinical care) | Operations (clinical care) |
| Clinical Trial | Yes | No |
| Regulatory Oversight | JHM sIRB (reliance agreement required) / PCORI / DSMB / CT.gov / etc. & Local Office of Telemedicine / Legal / ED | JHM Office of Telemedicine / Legal / ED |
| Randomization | Yes (cluster, stepped wedge design) | No |
| Consent Required | JHM sIRB (reliance agreement required) [follow-up consent for patients will be via mobile app and will occur post ED visit; local telemedicine rules apply for any additional consent required] | JHM Office of Telemedicine / ED (standard telemedicine consent) |
| Sites Involved |
~27 hospital EDs around the US affiliated with ~6 hubs, potentially includes JHM sites Note: EDs already running Tele-Dizzy cannot join the VERTIGO trial |
JHM (JHH or other adult JHM EDs); Outside JHM: any hospital willing to contract for the service with JHM (e.g., Allegheny General Hospital) |
| Interpretation of Results | JHM neuro-otologists (including potentially fellows or APPs prior to clinical attending review) OR certified local clinicians (neurology or EM) | JHM neuro-otologists (including potentially fellows or APPs prior to clinical attending review) |
| Billing / Finance | Site bills independently for testing; JHM delegates billing, paid per consult OR routine billing if locally interpreted | Site bills independently for testing; JHM clinicians bill directly for interpretation |
| VOG Goggles Used | ICS® Impulse – VOG running Otosuite software package (FDA approved) | ICS® Impulse – VOG running Otosuite software package (FDA approved) |
| Testing Personnel | Nurses or other clinical staff | Nurses or other clinical staff |
| Data Collection Tools | Tele-Dizzy software v2.0 (web-based, standard installer; local enterprise authentication is used at each site) | Tele-Dizzy software v2.0 (web-based, standard installer; local enterprise authentication is used at each site) |
| Direct Patient Video | As needed / available (e.g., Epic) | As needed / available (e.g., Epic) |
| Data Warehouse | JHM-managed Microsoft Azure instance (single PCORI-specific server for patients from all 27 sites) | JHM-managed Microsoft Azure instance (site-specific server for each health system / discrete entity) |
Why Tele-Dizzy is not research even though the VERTIGO trial is research
The video-oculography (VOG) technology used is FDA-approved and is currently in routine clinical use with human interpretation by neuro-otology experts. Tele-Dizzy uses store forward to digitally transfer the video images to the reader (and would be paired with video teleconsultation, as necessary). It is fundamentally no different than remote reading of fundus photos or radiographic images. It is standard expert clinical care provided by a remote means. Quality of image acquisition is monitored to ensure adequate testing is maintained, but this is no different than with tele-fundus photos or radiographs acquired remotely. Because there are video images of the room and eye, traces of the eye and head, and time-synchronized playback of the entire test result, monitoring quality is straightforward.
The VERTIGO Trial is designed to assess if diagnostic care based on clinical VOG interpretation (whether by remote experts or locally trained personnel) is superior to imaging-based diagnosis on diagnostic accuracy, diagnostic test utilization / ED length-of-stay, and health outcomes for patients with acute dizziness or vertigo in the ED. Thus, the VERTIGO trial is a research study assessing the impact of implementing clinical Tele-Dizzy. In the stepped wedge VERTIGO trial, sites will transition from imaging-based diagnosis (trial Epoch #1) to VOG-based diagnosis (trial Epoch #2). Since each care pathway will be designated as standard care at the time it is being given (i.e., there will be no patient-level randomization), consent will only be required for post-ED follow-up, done by mobile phone.
Partner With Us
We are actively recruiting hospital/ED partners to participate in a grant proposal for a 27-site comparative effectiveness trial we are submitting to the Patient-Centered Outcomes Research Institute (PCORI) in 2026.
The proposed V.E.R.T.I.G.O. Trial (Vestibular Emergency Room Teleconsults vs. Imaging for better diaGnostic Outcomes) compares video-oculography (VOG)-enabled teleconsults to a neuroimaging-first strategy to improve diagnosis of stroke vs. inner ear disease and associated health outcomes for adult ED dizzy patients. The full proposal is due May 5, 2026, and the trial is scheduled to run from March 2027 to February 2032.
We are looking for hospital and ED partners that meet these criteria:
- Are interested in learning more and are open to considering participation in the trial (note that the trial design is flexible enough to accommodate local needs/differences in trial implementation logistics).
- Can identify local personnel who would be interested in learning to perform VOG testing in the ED.
- Wish to explore this novel technology, which has the potential to improve quality of care, speed patient throughput/reduce ED length of stay, avoid unnecessary tests, reduce excess admissions to observation or inpatient units, decrease cognitive load for clinicians, and improve both patient and provider satisfaction.
If interested, contact us at [email protected].
References
Associated Press. $217 million awarded in malpractice case: A misdiagnosed Tampa man was left brain-damaged and disabled. Florida Times Union. 2006.
Badihian S, Sebestyen K, Keita M, et al. Trends in Imaging Utilization and Hospitalization of Dizziness and Vertigo in US Emergency Departments (1995-2015) [abstract]. American Neurological Association; 2020.
Edlow JA, Carpenter C, Akhter M, et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): Acute dizziness and vertigo in the emergency department. Acad Emerg Med 2023; 30(5): 442-86.
Fife TD, Iverson DJ, Lempert T, et al. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2008; 70(22): 2067-74.
ICS Impulse - 510(k) Number K151504. 2015. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K151504 (accessed December 13, 2020).
Kerber KA, Newman-Toker DE. Misdiagnosing dizzy patients: common pitfalls in clinical practice. Neurol Clin 2015; 33(3): 565-75.
Kerber KA, Schweigler L, West BT, Fendrick AM, Morgenstern LB. Value of computed tomography scans in ED dizziness visits: analysis from a nationally representative sample. Am J Emerg Med 2010; 28(9): 1030-6.
Natarajan EV, Aronson PL, Berkwitt AK. The cost of diagnostic delay and error. Hosp Pediatr 2021; 11(3): e38-e41.
Neuhauser HK. The epidemiology of dizziness and vertigo. Handb Clin Neurol 2016; 137: 67-82.
Newman-Toker DE, Keita M, Nassery N, et al. Total US societal costs of harms from diagnostic error estimated from malpractice and population-based data [abstract]. Diagnostic Error in Medicine 2018. New Orleans, LA; 2018.
Newman-Toker DE, McDonald KM, Meltzer DO. How much diagnostic safety can we afford, and how should we decide? A health economics perspective. BMJ Qual Saf 2013; 22 Suppl 2: ii11-ii20
Newman-Toker DE, Nassery N, Schaffer AC, et al. Burden of serious harms from diagnostic error in the USA. BMJ Qual Saf 2024; 33(2), 109-20.
Newman-Toker DE, Peterson SM, Badihian S, et al. Diagnostic Errors in the Emergency Department: A Systematic Review. Rockville, MD: Agency for Healthcare Research and Quality, 2022.
Saber Tehrani AS, Coughlan D, Hsieh YH, et al. Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med 2013; 20(7): 689-96.
Schwartz A, Weiner SJ, Weaver F, et al. Uncharted territory: measuring costs of diagnostic errors outside the medical record. BMJ Qual Saf 2012; 21(11): 918-24.
Smith M, Saunders R, Stuckhardt L, McGinnis JM, eds. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Washington, DC: National Academies Press (US); 2013.
Missed Stroke Diagnosis - John Michael Night's Story. 2020. https://www.improvediagnosis.org/stories_posts/missed-stroke-diagnosis/ (accessed February 12, 2020).
Tarnutzer AA, Gold D, Wang Z, et al. Impact of Clinician Training Background and Stroke Location on Bedside Diagnostic Test Accuracy in the Acute Vestibular Syndrome - A Meta-Analysis. Ann Neurol 2023; 94(2): 295-308.
Tarnutzer AA, Lee SH, Robinson KA, Wang Z, Edlow JA, Newman-Toker DE. ED misdiagnosis of cerebrovascular events in the era of modern neuroimaging: A meta-analysis. Neurology 2017; 88(15): 1468-77.