
Nerve Transfer
Nerve transfers can help restore function after certain types of nerve injuries.
What is a nerve transfer?
A nerve transfer is a procedure during which a surgeon takes a healthy, redundant, functioning nerve (donor nerve) and reroutes it to connect to a nonfunctioning, damaged nerve (recipient nerve). This allows nerve fibers (axons) from the donor nerve to grow through the recipient nerve. As the axons regenerate, the damaged nerve regains its ability to carry movement and sensation signals to the muscle or area of the skin it connects to. The goal of a nerve transfer is to restore function to the muscle or sensation to the skin that was lost due to nerve damage.
Without a healthy nerve stimulating the muscle, muscle fibers can quickly degrade (atrophy). This process is irreversible, so quick action is needed to save the muscle. A nerve transfer can often be performed close to the paralyzed muscle, so the nerve fibers have less distance to cover and the function can sometimes be restored sooner than with other procedures.
Nerve transfers offer an alternative to other methods of nerve repair, such as nerve grafting (when a surgeon takes a piece of a nerve from somewhere else) and direct nerve repair (when a surgeon reconnects the ends of a damaged nerve).
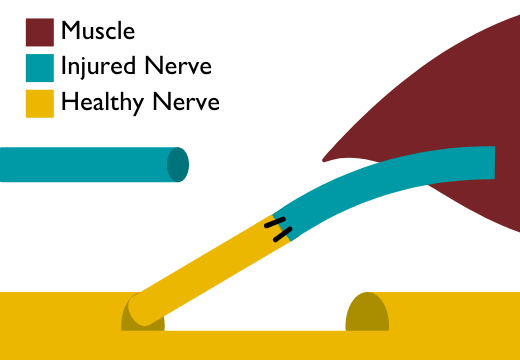
A simplified diagram of a nerve transfer
Who can benefit from nerve transfer surgery?
Nerve transfer is one of several surgical options for nerve repair. Whether you are a candidate for this procedure depends on the type and location of the injury. Nerve transfers can be a preferred treatment for:
- Nerve injuries that are farther away from the muscle supplied by the injured nerve. These injuries could include damage of the brachial plexus nerves in the shoulder and arm, as well as damage of a nerve in the pelvis, thigh or upper leg.
- Nerve injuries in which a long segment of a nerve is damaged or missing. Nerve transfers tend to provide better recovery of function in this case, compared with long nerve grafts.
- Older nerve injuries that scarred over and will not benefit from other repair methods, such as a nerve graft or muscle and tendon transfer.
- Cases when a nerve is damaged in a way that it cannot be reconnected and is unlikely to regenerate.
Peripheral Nerve Surgery at Johns Hopkins
Our experts at the Johns Hopkins Peripheral Nerve Surgery Center are well-versed in all types of nerve repair, including nerve transfers and nerve grafts. We use a holistic approach, creating an individualized treatment plan for each patient.
Nerve Transfers for Patients with Spinal Cord Injury
Nerve transfers can be used to restore muscle function in patients with spinal cord injuries in the neck (cervical spinal cord injuries) that lead to loss of function in some of the arm, hand or shoulder muscle groups.
In this case, the surgeon can use functioning nerves that branch off from the spinal cord above the level of the injury to serve as donor nerves. These donor nerves are transferred to nonfunctional recipient nerves below the level of injury.
Nerve transfers for treatment of spinal cord injuries use the same principles as nerve transfers for treatment of peripheral nerve injuries. One major difference is that nerve transfers can often help patients with spinal cord injuries many years after the injury. Unlike peripheral nerve injuries, spinal cord injuries usually do not cause irreversible muscle atrophy as time goes by.
For patients with spinal cord injuries, nerve transfer is one of many surgical options to address paralysis and spasticity (abnormal muscle tone and stiffness). Your surgeon might also recommend other surgical treatments, such as tendon lengthening, tendon transfers, joint releases and joint fusions. He or she will tailor the best combination of procedures to address your specific functional limitations and treatment goals.
What is the difference between a nerve transfer and a nerve graft?
With a nerve graft, a segment of sensory nerve tissue is taken from another nerve in your body (called autograft), processed/sterilized from a cadaver (called allograft) or grown artificially. The segment is surgically added to the damaged nerve to bridge the gap between its two ends. Nerve fibers regenerate across the graft to resupply muscles and skin that lost function or sensation.
With a nerve transfer, one of your own healthy nerves is cut and connected to the end of the injured nerve. And the nerve fibers from the donor nerve are rerouted into the recipient nerve. This process is similar in concept to a railway switch that routs trains to different destinations. There are benefits to this approach over a nerve graft:
- Faster recovery of function: While the growth of nerve fibers happens at the same speed (about an inch a month) regardless of which repair method is used, the distance from the repair site to the muscle varies. A nerve transfer is often performed closer to the paralyzed muscle, so the nerve fibers have a shorter distance to regenerate. A nerve graft is performed at the site of the injury, which may be further from the muscle, hence a longer distance to regrow and slower recovery of function. Because a muscle degrades (atrophies) over time without the nerve supply, it is essential to restore the connection as quickly as possible to maximize the amount of muscle function that can be restored.
- Better nerve supply: Nerve transfers often result in a greater number of nerve fibers reaching the affected muscle than is possible with a nerve graft. This, in turn, results in better muscle function.
How does a surgeon choose which nerve to transfer?
There are several factors that guide the surgeon in choosing the best nerve to transfer to the injured nerve:
- Nerve function: Nerves that are transferred (donor nerves) are usually redundant or nonessential. Because other nerves perform the same function as the donor nerve, you typically do not notice any functional loss resulting from the nerve transfer procedure.
- Proximity to the injured nerve: The donor nerve must be located close enough to the injured nerve to allow for the two nerves to be connected during the nerve transfer procedure. If there are no healthy, redundant nerves near the injured nerve, it is impossible to perform a direct transfer. In rare cases, it may be possible to transfer the donor nerve to the recipient by using nerve grafts.
- Similarity in muscle function: It is ideal if the donor nerve supplies a muscle with a similar or complementary function to the one that it is being reassigned to. This makes it easier for the patient to relearn how to control the muscle now that it has a different nerve supplying it.
- Similar number of axons (nerve fibers): Nerves may contain motor axons, sensory axons or both. Connecting nerves with similar composition helps ensure proper function of the repaired nerve.
- Similar size: Matching nerves of similar diameter makes it easier to surgically connect them and avoid scar tissue or neuroma development.
What are some examples of nerve transfers?
New nerve transfer procedures are being documented every year. Each transfer is different in the way it addresses a specific functional issue for a patient. Even transfers between the same nerves can lead to different results, as they might be performed in different places along the nerve’s length and surgeons may use different methods to connect the nerves.
Some examples of nerve transfers include:
- In the upper arm: Median and/or ulnar nerves are transferred to the musculocutaneous nerve to restore elbow flexion (bending the elbow toward the body). Read details below under Double Fascicular Transfers.
- In the forearm: median nerve to radial nerve transfer to restore wrist, finger and thumb extension (straightening).
- In the hand: ulnar nerve to median nerve transfer to restore thumb opposition (being able to touch the thumb to other fingers).
- In the upper leg: sciatic or obturator nerve to femoral nerve transfer to restore knee extension (straightening).
- In the lower leg: combined tendon and nerve transfers to restore ankle dorsiflexion (the opposite of pointing your toe) in patients with injured peroneal nerve (foot drop).
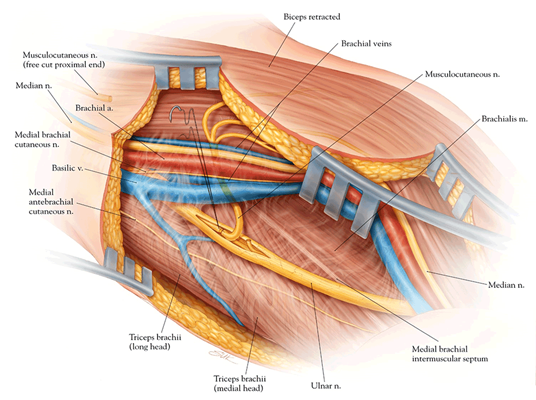
An illustration of a nerve transfer between a healthy fascicle of the ulnar nerve (donor nerve) and the poorly functioning or nonfunctioning musculocutaneous nerve (recepient nerve)
Double Fascicular Transfers
Sometimes, a nerve transfer could involve two nerves transferring parts of their functions to the damaged nerve. This is called a double nerve transfer or double fascicle nerve transfer. A fascicle is a branch of nerve fibers within the nerve responsible for specific functions.
For example, patients with brachial plexus injuries where the musculocutaneous nerve in the arm is injured may be unable to bring the lower arm to the body by flexing the elbow. In this case, parts of the nearby nerves (ulnar and median) can be rerouted to restore this function.
Nerve Transfer Surgery Risks
- As with any surgery, there is a risk of infection after a nerve transfer.
- There is also a small risk of injury to the donor nerve, which can lead to partial loss of function.
- There is a chance that a nerve transfer is not successful in addressing your symptoms, and that may limit your future treatment options.
Recovery After Nerve Transfer Surgery
Recovery after a nerve transfer has two parts: healing of the tissues disrupted during the surgery and restoration of the lost function. While tissues may heal fairly quickly, it may take some time for the nerve to regrow, and may sometimes involve working with physical or occupational therapists to restore movement and sensation in the affected limb.
The transferred nerve fibers need time to grow into the new pathway established during the transfer. And your brain needs time to adjust to supporting the new function of the transferred nerve. It may take several weeks to several months to recover after a nerve transfer. But restoration of function may be faster than after a nerve graft procedure that requires a longer segment of nerve fibers to regenerate.
Pain from the incision site is usually minimal and is temporary. If you had pain from the nerve injury, it is also usually minimal after the surgery and can be addressed with over-the-counter pain medications while your nerves heal.
Nerve Transfer Success Rate
The success of a nerve transfer is determined based on how well the procedure restores your function and helps reduce pain and other symptoms. Success depends on the type and severity of your nerve injury and the skills and experience of your surgical team. Between 80% and 90% of patients with brachial plexus injuries tend to experience significant improvement after a nerve transfer.

