As spring brings blooming flowers and longer, brighter days, Adam Kaplin’s thoughts turn to darker subjects. The Johns Hopkins assistant professor of psychiatry and behavioral sciences focuses on depression and suicide.
He knows that, contrary to popular belief, suicide rates spike in the light of spring, not the darkness of winter.
“In April, May and June, the suicide rate goes up and is the highest,” Kaplin says. Those numbers can be two to three times higher than in December, when suicide rates are the lowest.
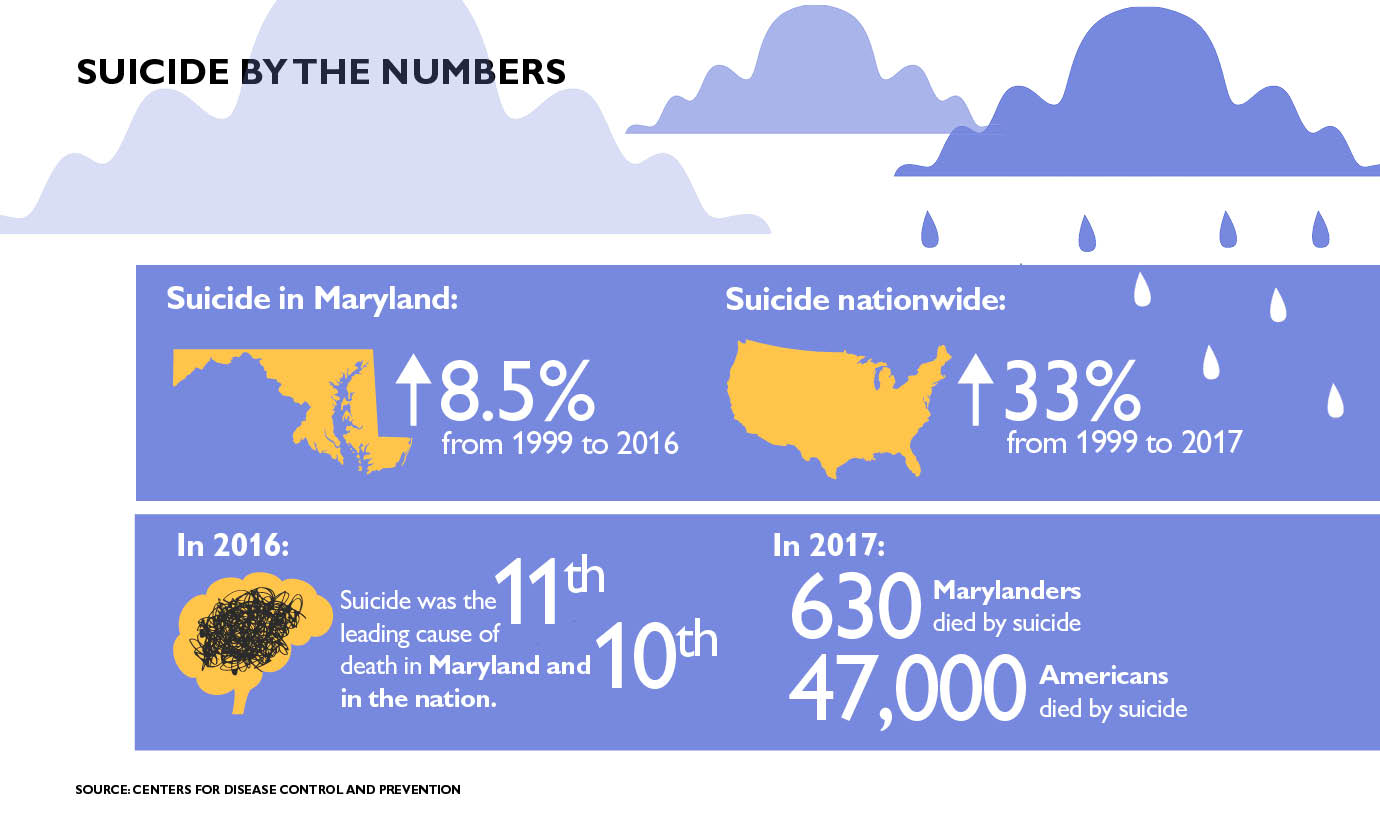
In 2017, suicide was the 10th leading cause of death in the United States. More than 47,000 people took their own lives. Kaplin monitors about 300 of his patients — and with increased attention this time of year — via an app he created with Remedy Health called Mood 24/7, an automated texting service that asks patients how they’re feeling once a day. The app has about 15,000 users.
“I can look it up online and see how they’re doing in real time,” he says. “I more closely monitor those things in the spring.”
Kaplin recently spoke with Dome about the seasonal nature of depression and suicide.
Q: What does science say about this phenomenon?
A: Overwhelming evidence suggests that inflammation from various sources, including allergic reactions, can cause or worsen depression. Our immune system spends the winter trying to ward off viral infections, but not trying to ward off allergies, which affect more than 50 million Americans each year. Seasonal allergies in the spring put a large number of Americans at a higher risk for depression.
Q: How much higher is that risk?
A: Johns Hopkins otolaryngologist Sandra Lin, who specializes in allergies, is co-author of a study soon to be published in The Journal of Allergy and Clinical Immunology that shows the odds of depression are significantly higher in those with rhinitis, the symptoms of which include a stuffy or runny nose, sneezing and postnasal drip. The chances of depression were 42% higher in people with rhinitis (both allergic and nonallergic) than those without.
Q: You treat patients with multiple sclerosis. Are patients with autoimmune diseases more prone to depression?
A: All the autoimmune diseases that we know of have higher rates of depression. In multiple sclerosis, which I study, suicide is the third leading cause of death in patients, compared with the 10th leading cause of death in the general population. Other autoimmune diseases such as rheumatoid arthritis, Crohn’s disease, diabetes and lupus also have elevated rates of depression.
While these diseases can cause depression, depression is also a risk factor for diagnosis with an autoimmune disease.
Q: Is inflammation elevated in patients with depression?
A: Yes. People who have depression from unknown causes without an autoimmune disease have elevated levels of inflammation compared with people who don’t have depression, but the levels are not nearly as high as in those with an autoimmune disease. In the case of patients with MS, we have evidence that blocking inflammation also helps treat depression.
Q: Do other seasonal factors contribute to the higher rate of suicide?
A: I believe that those who may have spent the winter depressed find themselves, in the spring, still depressed, but with the energy and motivation to take their own life.
I also think spring is particularly tough for people who are depressed because after a largely solitary winter, those people emerge into a world full of rebirth, rejuvenation and revelry. In contrast, they feel dark and sad.
Q: What happens to the suicide rate after the spring?
A: For the most part, the peak is in the spring and summer and then it goes down and down until December, when it’s the lowest. We see the fewest reported attempts and fewest new psychiatric appointments in December.
Q: Is the spring peak in suicide reflected in your patients who are on the Mood 24/7 app?
A: It is not, because it’s a relatively small cohort. Even though tens of thousands of people die by suicide, it is still a relatively rare thing given the millions of people who are depressed. For every 300 people who have suicidal thoughts, 30 will attempt suicide and only one of the 300 will complete suicide.
When patients have commented on being suicidal, I’ve gotten them into the hospital and prevented them from harming themselves.
Q: Is the spring peak in depression affected by geographical latitude?
A: Yes, absolutely. The peak is less pronounced closer to the equator, where there are less seasonal differences. Some studies show more spring suicides in places farther from the equator.
Q: Do climate change and pollution play a role in suicide and depression?
A: There is mounting evidence that says pollution is bad for your mental health. We know it’s bad for your health in general. Climate change — and the extreme weather it brings — also appears to be a factor. A number of studies say that even when you remove seasonality from the equation, with 10 hot days in a row, you have higher rates of suicide.
Q: How does the psychiatric department at Johns Hopkins handle mental health emergencies?
A: My department provides 24/7 psychiatric coverage of the emergency department. Because mental health is such a prominent issue, psychiatry is the only specialty that has its own wing in the emergency department devoted to treatment and placement in either The Johns Hopkins Hospital or another institution.
To read more, visit hopkinsmedicine.org/health/conditions-and-diseases/depression-and-suicide.