TULSA Gives New Options for Intermediate-Risk Prostate Cancer
A new procedure gives patients a treatment option with fewer side effects.
For patients with intermediate-risk, localized prostate cancer, Johns Hopkins offers MRI-guided transurethral ultrasound ablation (TULSA), which can target the tumor and preserve sexual function and urinary continence.
The outpatient procedure is performed with the patient under general anesthesia, which allows surgeons to treat the cancer with millimetric precision, thanks to MRI guidance. Johns Hopkins is the first in the Greater Washington and Baltimore region to offer the procedure commercially, and participated in the pivotal trial that led to the device’s FDA approval.
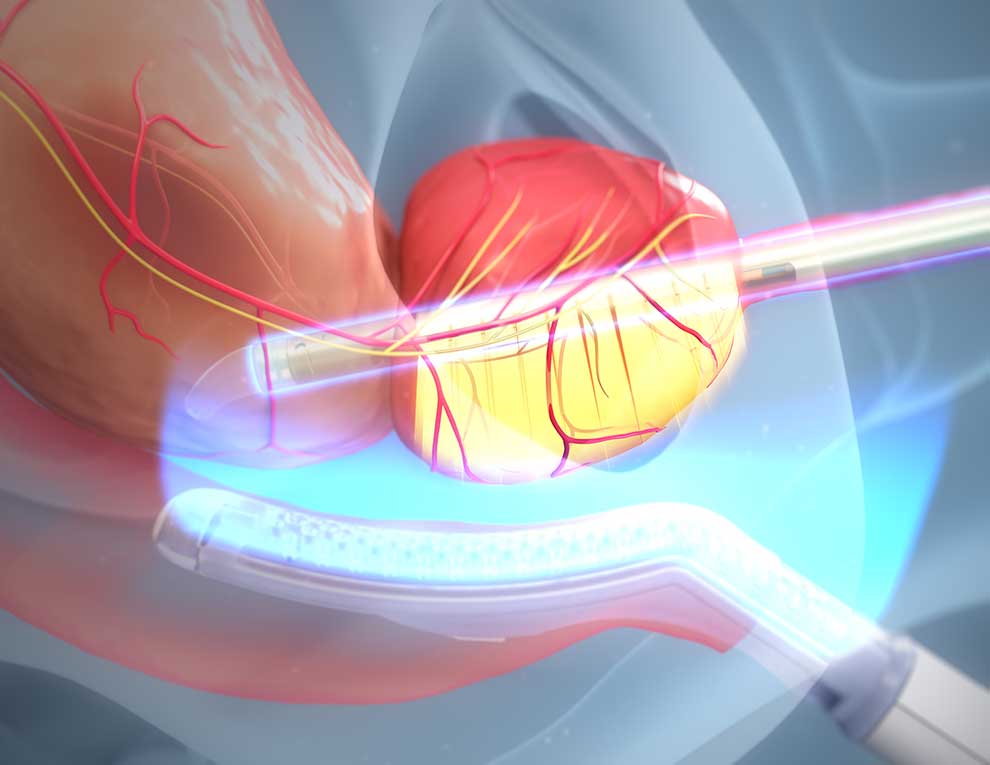
During TULSA, a urologic surgeon inserts a urethral applicator similar to a rigid cystoscope into the urethra, as well as a separate rectal cooling device into the rectum, then puts the anesthetized patient into an MRI machine. With MRI guidance, the surgeon can adjust the applicator and make sure the cooling device is in the right place as well.
The applicator is equipped with up to 10 parallel, 5-millimeter-thick sections that beam out waves of high-intensity ultrasound from the apex to the base of the prostate. The unit can rotate 360 degrees to target the necessary prostate tissue. Throughout the procedure, there is active cooling of the urethra and rectum, as well as MR thermometry to monitor temperatures of the prostate, urethra and rectum.
“Because the patient is on the MRI table, they can have a diagnostic MRI scan post-procedure to determine whether we treated all the areas that we planned on treating,” says urologic surgeon Arvin George. “You have multiple layers of feedback.”
Patients are sent home with a catheter, which can be removed within a week or two. Because TULSA treats the prostate from the inside out, George says, there is more opportunity to preserve the nerves involved in sexual function.
“By using MRI, we harness both the unique detail of a patient’s prostate anatomy and the automatic control of treatment parameters,” says radiologist Katarzyna Macura. “By using this imaging-based approach, we apply precision into planning the treatment, targeting the cancer, and preserving critical structures to optimize functional outcomes.”
A multidisciplinary procedure, TULSA involves specialists from urology, radiology and anesthesiology, as well as an MRI technologist. Urological oncology fellows and other members of the urology research team are often involved as well.
Patients who are good candidates for TULSA include those with a Gleason score of 7 whose cancer is confined to the prostate and who have no calcium deposits in their prostate.
Johns Hopkins was a research site for a multisite clinical trial that led to the FDA’s approval of the device in 2019. The TACT (TULSA ablation clinical trial), published in 2019, involved 115 men with low- and intermediate-risk prostate cancer who had whole gland ablation.
At one year, 65% of trial participants had negative biopsies, with clinically significant disease decreasing from 85% of participants before treatment to 20% after. At five years, only 21.7% of men had undergone salvage treatments for recurrent prostate cancer, and the remainder were being monitored by their urologists, as patients are after any prostate cancer therapy.
Urologic oncologist Christian Pavlovich, principal investigator for the Johns Hopkins TACT trial site, notes that with these results, TULSA can’t quite compete with radiation or surgery for cancer control, but the very minimal side effects were one of TULSA’s big advantages.
“There were very few patients who had significant long-term side effects,” says Pavlovich. “Most patients [who receive other treatments] have at least transient ED and urinary incontinence — either of which can persist in some patients — but after prostate ablation, we didn’t see much of either. There were very few long-term impacts noted in the major TULSA trials because you can confine the ablation to the prostate itself.”
There is a second ongoing trial, CAPTAIN (customized ablation of the prostate with the TULSA procedure against radical prostatectomy treatment), which is comparing the two procedures in terms of erectile dysfunction, urinary continence and whether patients need additional treatment, and for which Johns Hopkins is also a research site, with Pavlovich serving as PI.
Medically reviewed by Katarzyna Macura, M.D., Ph.D., and Christian Pavlovich, M.D., April 10, 2026.
For Clinicians Clinical Connection
Clinicians, discover the latest in research and clinical innovation from Johns Hopkins experts. Access educational videos, articles, CME courses and other resources from our world-renowned institution.