Fluorescent Imaging Breakthrough Helps Johns Hopkins Surgeons Target Hidden Lung Tumors
Surgeons at The Johns Hopkins Hospital are the first in Maryland to use the product.
Surgeons at The Johns Hopkins Hospital are the first in Maryland to use a fluorescent imaging technology that helps them locate and remove hard-to-find lung tumors during minimally invasive thoracic surgeries, potentially improving outcomes while reducing recovery time and complications.
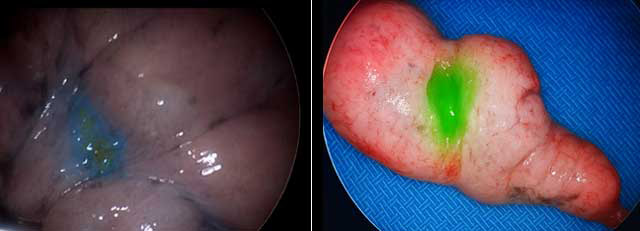
During surgery, fluorescent imaging highlights a lung nodule that wasn’t visible by the eye (left). After the procedure, imaging confirms the nodule was successfully removed (right). | ©2025, Johns Hopkins Medicine.
The technology, approved by the Food and Drug Administration in November 2021, is unusual in that it specifically targets tumors, even ones that are small or below the surface, by using an intravenous imaging agent that turns them a fluorescent green that’s visible through a specially equipped camera during laparoscopic surgery.
“We’re increasing the number of tools that we have to perform better cancer surgeries, with fewer complications,” says Jinny Ha, assistant professor of surgery and thoracic surgeon at Johns Hopkins.
“One of the challenges that we face in thoracic surgery is trying to find small lung nodules that are not on the surface,” she says. “This goes directly to the targeted cells and nothing else, so it is specific and binding to that nodule, lighting it up for us.”
Ha and thoracic surgeon Stephen Yang, professor of surgery at the Johns Hopkins University School of Medicine, are the first in Maryland to use the product, which has the generic name pafolacianine and is also approved for ovarian cancer. It works by binding selectively to cancer cells, enabling surgeons to clearly visualize and remove tumors that would otherwise be invisible or inaccessible.
Unlike a static image from a CT scan, the fluorescence-guided system gives surgeons dynamic, real-time visual cues that adapt with each breath.
“If I’m using a CT scan as my map, then intraoperatively I’m looking at a deflated lung, which is totally different,” Ha says. “I have to rely on my understanding of anatomy to help guide where potentially in this lung is this nodule. It’s particularly challenging if it’s small or if it’s not on the surface. We also don’t want to dissect areas that don’t need dissection. This really eliminates that stress.”
Thoracic surgery is moving toward robotic and minimally invasive procedures, she says, which are easier on the patient, with faster recovery and less risk of complications. However, Ha notes, minimally invasive techniques mean “our ability to physically feel the lung tissue to find these nodules is not possible.”
Patients receive an intravenous infusion of the imaging agent one hour to 72 hours before surgery, either in an outpatient clinic or preoperatively. Surgeons then use a camera that’s specifically equipped to see the fluorescent light.
“The camera system hooks up to the screens that we use for robotic surgery or video-assisted surgery, and it’s a real-time assessment of the lungs,” says Ha. “It helps us see the targeted spots, and is also helpful for finding spots that we didn’t identify early on.”
Side effects from the agent are rare, but can include nausea. Most patients remain in the hospital two to three days to recover after surgery.
For Clinicians Clinical Connection
Clinicians, discover the latest in research and clinical innovation from Johns Hopkins experts. Access educational videos, articles, CME courses and other resources from our world-renowned institution.